Erin Poffenberger, Frederick County Infants and Toddlers Program, Frederick, Maryland
Abstract
Part C of the Individuals With Disabilities Education Act (IDEA) mandates the provision of early intervention (EI) services to qualifying children under 36 months old. Social–emotional development is one area that programs are obligated to provide assessment and intervention for and yet, most EI programs do not have licensed mental health professionals (MHP) on staff. This article highlights the need for the MHP as a member of the EI team and presents ways to expand their role to enhance the quality of EI services provided to children and families. The author describes how the EI program in Frederick County, Maryland, is using MHP in an innovative way.
Early nurturing relationships with parents and caregivers are crucial for infant and early childhood development. It is within these relationships that infants, toddlers, and young children build strong (or weak) foundations for cognitive, emotional, and social development. When parents are responsive, nurturing, and stable, infants, toddlers, and young children develop secure attachments, which allow them to become confident, resilient, and better able to manage their emotions.
Mental health professionals (MHPs) need to become staple members of the early intervention (EI) team in order to ensure that social–emotional delays are identified as early as possible. Providing mental health services to young children and their families within EI is vital. Without the expertise of the MHP on the EI team, these disruptions in healthy attachment are being overlooked and untreated. The Frederick County Infants and Toddlers Program (FCITP) located in Frederick, MD, is expanding the role of the MHP on the EI team to better meet the needs of children and families in the program.
Part C EI
Part C EI refers to services that are available to children younger than 36 months old through the United States’ special education law—the Individuals with Disabilities Education Act (IDEA). Eligibility for Part C EI services is determined by each state’s definition of developmental delay. Specific eligibility requirements vary from state to state, but generally, infants and toddlers are found eligible for services if they have been diagnosed with a physical or mental condition that has a high probability of delayed or atypical development. Examples include, but are not limited to, Down syndrome, visual or hearing impairment, extreme prematurity, epilepsy, and fetal alcohol syndrome. Infants and toddlers will also qualify for services if they present with a delay in at least one of five developmental areas (cognitive, physical including vision and hearing, communication, social or emotional, or adaptive; Centers for Disease Control and Prevention, 2018).
Most EI programs employ a multidisciplinary team, commonly consisting of physical therapists, speech–language pathologists, special educators, occupational therapists, and service coordinators. Less commonly, the EI team may include other licensed professionals such as psychologists, social workers, developmental pediatricians, or nurse practitioners.
Mental Health Support and Part C EI
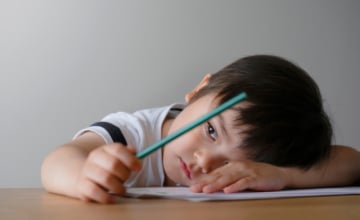
Receiving a diagnosis of a child’s disability can bring a range of emotions (e.g., shock, grief, anger, guilt) that are similar to those experienced when learning about the death of a loved one (Woodman et al., 2015). When compared to parents of typically developing children, parents of children with developmental disabilities are more likely to experience social isolation, stress, fatigue, marital distress, and lack of stable employment (Malone et al., 2000). In addition, these parents report higher rates of general ill physical health (e.g., headaches, musculoskeletal pain, sleep problems) and higher rates depressive symptoms (Masefield et al., 2020). MHPs are exceptionally qualified to help parents of children with disabilities process life-altering diagnoses and address their unique psychosocial needs.
MHPs are also uniquely qualified to address child development needs impacted by child maltreatment, parental mental health, and parental substance use. Analysis of data from the National Co-Morbidity Survey suggests that approximately one half of mothers (46.8%) and one third of fathers (29.5%) have had a psychiatric disorder at some point during their lifetime (National Academies of Sciences, Engineering, and Medicine et al., 2016). About 1 in 11 infants will experience their mothers’ major depression in their first year of life (Center on the Developing Child at Harvard University, 2009). Depressed mothers typically engage in fewer positive interactions and provide less developmental stimulation to their children (Center on the Developing Child at Harvard University, 2009). As a result, these children perform lower, on average, on cognitive, emotional, and behavioral assessments than children of nondepressed caregivers (Center on the Developing Child at Harvard University, 2009). COVID-19 has only exacerbated the mental health needs of parents. When compared to before the pandemic, parents have reported worsened mental health, increased alcohol use, increased suicidal thoughts/feelings, worsened mental health of their children, and an increase in negative parent–child interactions (Thomson et al., 2021).
Similar to mental health conditions, parental substance use and child maltreatment affect child development. Chronic substance use affects a parent’s ability to regulate their own emotions, to provide safe and consistent care for their child, and to be mentally alert for child bonding and intellectual development (National Academies of Sciences, Engineering, and Medicine et al., 2016). National data shows that 38%–65% of infants and toddlers encountered by child welfare agencies have delays and that 35% of these infants and toddlers would qualify for EI services at the time of contact with child welfare (Gilkerson et al., 2013).
This information is not novel. Researchers know that parental substance use and child maltreatment make children more likely to experience developmental delays. For this reason, additions to the Child Abuse Prevention and Treatment Act (CAPTA) legislation require states to establish procedures to refer children younger than 3 years with substantiated cases of child abuse or neglect to EI services (Young et al., 2009). Thirteen years ago, the Substance Abuse and Mental Health Services Administration warned that CAPTA legislation would increase the number of children that Part C would assess and that the needs of the children referred under CAPTA would be different than other children. Specifically, the agency advised that Part C would need to enhance its ability to address parental issues that affect children’s mental health, such as parental substance abuse, domestic violence, and parental mental health problems, especially maternal depression (Young et al., 2009). Unfortunately, 13 years later most EI programs are still not able to meet these needs.
Current Roles of MHPs in EI
As mentioned previously, the EI team is a multidisciplinary team that most commonly includes physical therapists, speech–language pathologists, special educators, occupational therapists, and service coordinators. MHPs, such as licensed clinical social workers or counselors, are not core members of EI teams. Many EI programs across the country do not have any staff members with expertise in family system dynamics, mental health, or social–emotional development. Programs that do have an MHP on the team may only have one available to service the needs of an entire county. Comparably, the same program might have 4 to 5 times as many physical therapists, speech–language pathologists, special educators, and occupational therapists to service the needs of the same county. Many MHPs in EI are forced to provide consultation and referral to outpatient counseling due to the overwhelming need for their services and lack of qualified staff available to meet those needs.
In December 2020, the Institute for Innovation and Implementation at the University of Maryland School of Social Work in collaboration with the Maryland State Department of Education, Division of EI and Special Education released a survey to directors of Maryland Part C Infants and Toddlers programs to ascertain agency capacity to implement infant early childhood mental health consultation services (Candelaria et al., 2021). Of the 24 counties that responded to the survey, half do not have designated staff in their programs to address infant and early childhood mental health or social–emotional concerns. The same survey identified that 66% of counties in Maryland screen and refer out for supportive services for infant and early childhood mental health or social–emotional concerns, yet only 9% said that there were sufficient support services in the community in which to refer (Candelaria et al., 2021). Referring out for mental health services for children in communities that do not have adequate mental health providers further stresses families in need. It is a duty and obligation to provide referrals for families to access professionals that will be able to provide the services and support they need. Sara, a mother of a child who received child–parent psychotherapy (CPP) through the FCITP, shared her thoughts on the efficacy of referral to outpatient counseling by EI programs. She explained,
A referral would have done more harm than good. I was in crisis and I needed someone to come to me. Working my way through a list trying to figure out who can get me in, who takes my insurance, who fits into my schedule, wouldn’t have helped me at all.

Mental health professionals are exceptionally qualified to help parents of children with disabilities process life-altering diagnoses and address their unique psychosocial needs. Photo: shutterstock/matuska
EI programs do not operate without key professionals such as physical therapists, speech therapists, and occupational therapists on staff, so why is it acceptable for EI programs to operate without MHPs on the multidisciplinary team? There is a critical gap in EI in access to services for one of the five domains providers are mandated to serve (social–emotional development). This gap does not exist in the same way for more obvious needs such as speech or motor delays. Are social emotional and mental health needs less obvious? Harder to evaluate? More stigmatized? Harder to treat? Regardless of the “why,” it is clear that EI programs do not have nearly enough, if any, qualified MHPs to meet the needs of the population in the same way they are staffed to meet the needs of other developmental delays.
Vision in Action
FCITP director Lisa Jarboe was becoming increasingly aware of the mental health needs of infants, toddlers, and their families and set out to pursue a different vision for how to use MHPs in Frederick County EI. Historically, Frederick County’s EI program has had only one social worker on staff to service the entire county. Because this was such a limited resource, social work services to families focused on parent training strategies to manage challenging child behavior. Infant and toddler mental health concerns and parental mental health concerns were not addressed in the service plan, and families were given referrals for outpatient counseling options for these needs. Lisa advocated to add a social worker position to the FCITP team and collaborated with this writer to change the way this position supports staff and families.
Changes in FCITP began with an investment in professional development trainings in infant and early childhood mental health for the MHPs. Most licensed MHPs do not have specialized training in early childhood mental health. These trainings are costly, preventing individuals from accessing them independently. In 2019, Frederick County Safe Babies Court Team generously provided funding for two licensed clinical social workers from FCITP to begin an 18-month CPP Learning Collaborative. In addition to CPP, FCITP has also invested in the Infant and Early Childhood Mental Health Certificate Program through the University of Maryland School of Medicine.
With support from leadership and funding for trainings, FCITP has used their MHPs to provide professional development opportunities to staff. This began with broadening the awareness of the EI team regarding the scope of what MHPs can address within EI. Some disciplines less familiar with working alongside of MHPs might find terms like “social worker” analogous to “case worker” and not know how a clinical social worker can be used in the diagnosis and treatment of child and adult mental health disorders. Once FCITP staff were more familiar with the scope of the MHPs’ practice expertise, the MHPs developed specific professional development trainings based on topics of interest and recurring themes identified from team meetings. Some of these topics for professional development trainings included: the impact of trauma on development; working with caregivers with anxiety and depression; assessing, analyzing, and intervening to address challenging behavior; motivational interviewing; and the stages of change and their relation to working with families.
FCITP EI providers use the MHPs for consultation purposes. The role of the MHP as a consultant is not novel as many EI programs use an MHP for information about concrete resourcing needs (e.g., housing, transportation, financial resources, support groups). In FCITP, the MHPs are also used for consultation regarding general provider practices. For example, FCITP MHPs have been consulted regarding the appropriate use of self-disclosure during the delivery of home visiting services, how to recognize and respond to compassion fatigue and burnout, how to have challenging conversations with families (e.g., processing significant delays or suspected developmental conditions that have not yet been diagnosed), how to build rapport with families of different backgrounds, and building awareness of external factors that impact a family’s perspective and progress.
In addition to the role of consultant, FCITP MHPs are also direct service providers. Like in many programs that employ MHPs, they may be added to an individualized family service plan (IFSP) to provide parent training to improve a parent’s ability to manage challenging child behavior. Parent training services can adequately address the needs of some children and families, but will not be enough to make a meaningful difference in the lives of families with more intense or complex needs. For these families, FCITP also uses the MHP as the provider of psychotherapeutic services. FCITP MHPs have provided psychotherapy to parents and caregivers when the adults’ mental health needs were inhibiting child progress. In addition, CPP has been provided to children whose development has been impacted by abuse, neglect, or other traumas. The provision of CPP either in isolation or alongside an additional EI service such as speech therapy, occupational therapy, or physical therapy has assisted in moving these children closer to a typical developmental trajectory. The next sections present two case studies, both highlighting a different way an MHP was used to provide psychotherapeutic services to just a caregiver and also a child–caregiver dyad. Some names have been changed to protect family’s choice of confidentiality.
Tiffany’s Story
Tiffany began her relationship with FCITP when her son was 18 months old, after he was found eligible for EI services due to an expressive language delay. The initial service plan included a blend of child-level outcomes, which focused on increasing his ability to use verbal communication to express wants and needs, as well as family-level goals focused on weaning from breastfeeding and establishing sleep routines. A speech–language pathologist began services with the family at a frequency of 3-4 sessions per month. Seven months after initiating services, the speech–language pathologist referred Tiffany to the EI MHP following an emotional home visit. Tiffany recalls this experience:
As the visits with my son’s appointed speech therapist progressed, we grew closer to her. It was quick and easy because she was right in our home, and she was always such a genial and uplifting presence. One morning, during our scheduled weekly visit, we had just received the tragic news my husband’s grandmother had passed away overnight. I was so distraught we didn’t have any dependable child care so that I could accompany my husband to the funeral that I just started crying and couldn’t stop. Everything came pouring out to the speech therapist—my anxiety about virtually everything in my life, my guilt about why my youngest son didn’t talk and how my eldest son was likely autistic, my shame telling myself if I was just a better mom my children wouldn’t have these challenges. At that moment she felt like the only support we had. She listened to me cry and was so empathetic she teared up herself. She hugged me and asked me if it was okay if she had the program’s clinical social worker reach out to me to provide mental health support. I was nervous but agreed. At that point she had gotten to know us so well she knew I had a really hard time making phone calls and told me she’d have the social worker reach out to me by email.

Referring out for mental health services for children in communities that do not have adequate mental health providers further stresses families in need. Photo: shutterstock/polkadot_photo
Social work services were added to the service plan at this time, and the MHP began seeing Tiffany weekly for individual counseling in addition to the speech therapy services provided by the speech–language pathologist. The MHP used a psychodynamic approach to treatment infused with elements of cognitive behavioral therapy. Treatment goals focused on: (1) decreasing feelings of guilt and responsibility related to children’s diagnoses, (2) decreasing intrusive anxious thoughts, (3) completing evaluation and connection to treatment for Tiffany’s 10-year-old child, (4) increasing readiness to connect with a psychiatrist for medication management to manage Tiffany’s anxiety and depression, (5) increasing Tiffany’s social support network and (6) improving self-esteem and confidence advocating for children’s treatment needs. Social work services for individual counseling were provided for more than 2 1⁄2 years (gradually spacing out the frequency to prepare for termination of services) until Tiffany’s son was no longer eligible to continue on an extended IFSP due to his age. Maryland, Connecticut, and the District of Columbia are the only territories in the United States that allow families of eligible children the option to extend EI services through an IFSP after the child reaches 3 years old until the beginning of the school year following the child’s fourth birthday. When Tiffany’s son turned 3 and was deemed to be eligible to continue services, Tiffany chose to continue services with FCITP on an extended IFSP rather than transition to an Individualized Education Program (IEP). Tiffany made this decision based on her value of the mental health counseling she was receiving from FCITP, a service that would not be provided by the school system if she transitioned to an IEP. Tiffany reflected on her experience receiving mental health counseling through FCITP:
When I met with the Infants and Toddlers mental health clinician for the first time, I admitted I had struggled with anxiety and depression my whole life but had never gotten any type of successful treatment. She was so easy to talk to and she recognized the struggles I was going through as a mother of two children who have higher support needs. In the over 3 years we met regularly, she has helped me work through crippling anxiety, bouts of debilitating depression, past trauma, low self-esteem, and the overwhelming feelings of guilt I struggled with surrounding my children’s developmental delays. She taught me coping strategies when I have intrusive thoughts and how to process and communicate my feelings more effectively. She helped me build the confidence to advocate for my children and offered guidance through my older son’s autism diagnosis. She recommends resources without pressure. She helps me find my courage when I have self-doubt. She never rushes me. She never judges me the way I judge myself. She reminds me to reach out to her if I’m having a bad day. She celebrates my accomplishments no matter how small they may seem. She motivates me to be the best version of myself not by demand or duress, but by equipping me with the tools to create my own self-acceptance and realize my self-worth. She has had a profoundly positive impact in not only mine but my whole family’s lives. I am so grateful.

Parent training services can adequately address the needs of some children and families, but will not be enough to make a meaningful difference in the lives of families with more intense or complex needs. Photo: shutterstock/Iryna Imago
I want to be as clear as I can. The Frederick County Health Department’s Infants and Toddlers Program changed my life. My husband and I went from feeling scared and alone to being surrounded by a team of people who cared, and it didn’t even cost us anything. The support from every staff member we’ve ever interacted with has been invaluable, but the mental health support I’ve personally received has by far been the most impactful. I cannot stress enough how essential this support is to families in EI programs, and I wholeheartedly believe it has exceedingly contributed to the success of my son’s development.
Because of the mental health support provided by the Frederick EI program, my children have a healthy and happier mom, their parents have a stronger union, and we are all thriving better than ever.
Ava’s Story
Ava’s Department of Social Services worker referred her to the FCITP at 4 months old due to overall developmental concerns. Ava was born 33 weeks gestation and spent 19 days in the neonatal intensive care unit to manage issues associated with prematurity and respiratory distress. Ava qualified for services based on a 25% delay in adaptive development. Her foster mother expressed concerns related to feeding and regulation. Specifically, Ava would become hysterical during bath time and often took hours after bath time to settle. Ava also had difficulty coordinating sucking, swallowing, and breathing during feedings. Initial services provided by FCITP included physical therapy, occupational therapy, and infant massage. Initial outcomes focused on exploring sensory strategies to assist with soothing, relaxing muscle rigidity, and improving coordination with feedings. Ava continued to receive services from an occupational therapist for the next 11⁄2 years. During that time, Ava experienced various psychosocial changes including supervised visitation with biological family members that was characterized as stressful and chaotic, a change in foster placement to a new foster family that would later become her adoptive family at 10 months old, and the sudden death of a biological parent. Services with the occupational therapist focused on Ava’s self-regulation and motor skills. Ava continued to experience a variety of difficulties that were not fully resolved with sensory support strategies. Due to her traumatic family history, the occupational therapist consulted with the MHP to help determine if additional factors could be contributing to Ava’s challenges.
The MHP joined the occupational therapist at the family home for a joint visit right after Ava’s 2nd birthday. Her adoptive mother, Sara, shared preliminary information about her concerns related to Ava’s poor quality of sleep, frequent tantrums, and emotional dysregulation throughout the day. In addition to occupational therapy services through FCITP, Ava was also receiving outpatient occupational therapy and speech services. Ava and Sara also had a few sessions with an outpatient trauma therapist who reportedly tried some eye movement desensitization and reprocessing and bilateral tapping techniques that Sara reported did not have any impact. The MHP provided an explanation of CPP and its efficacy with treating trauma in children under 5 years old. Sara was enthusiastic to begin CPP, and social work services were added to Ava’s IFSP. Sara, like Tiffany, elected to remain on the extended IFSP to continue receiving services from FCITP rather than transition to a school-based IEP. This decision was largely based on her ability to continue accessing CPP, a service that would not be available to her on an IEP. Sara reflects on her experience receiving CPP through FCITP:
Prior to beginning CPP we already had so many evaluations and services from medical doctors, [occupational therapists], [physical therapists], special educators, and speech therapists but something was missing. Everyone was helping with pieces of the puzzle, but it was as if everyone was looking only at their piece, through their lens. Until we met Lauren, no one had mentioned that maybe trauma was contributing to Ava’s challenges and that we should pull in a provider with expertise in this area. I was intrigued. I was aware of CPP and its efficacy for children who have experienced trauma, but it was not something I ever thought we would have access to through EI. CPP was definitely the missing piece for my child and family. It was not until we started receiving CPP, alongside of our other EI services, that I felt like we were starting to crack the code for Ava. The benefits I experienced from participating in CPP through our EI program are hard to put into words but I will try my best. As a parent, I have a better understanding of when and why I am being triggered by my child’s behavior. This awareness allows me to take a step back and regulate myself first before I respond during times when Ava is really struggling. I am less anxious and I respond from a more patient, regulated place. I feel more empowered as a parent. I have greater awareness of things that might trigger Ava and feel confident in my ability to either prepare her for it or help her soothe thereafter if it cannot be avoided. Because of CPP, I have developed the skill of being able to talk to my child about important, difficult things like death and trauma in a way that she can understand them. The length of time I received CPP might have been short in the grand scheme of things, but I was given the tools to understand, interact, and communicate with my child that I will be using for the rest of my life. Had I not had access to a MHP through my EI program we probably would have given up. Her tantrums, sleep challenges, and dysregulation were so extreme. We were at a place where we had tried so many things and had been given so many tools that didn’t work that I felt defeated. We needed someone with an expertise in trauma to help us meet our IFSP goals.
What Do Other Service Providers Think?
In addition to the benefits reported by caregivers, service providers value the MHP as a member of the EI team. Several service providers in FCITP were asked to provide their reflections regarding the MHPs on their teams.
I’m not comfortable addressing social–emotional/mental health needs of children and caregivers on my own. Having access to mental health resources pales in comparison to having an MHP on my team. Our MHPs have been able to answer my questions immediately and consult with me about specific situations. Without their input, guidance, and expertise, I would not be able to effectively meet the needs of many of the children and families I serve. The MHP helped me learn and implement boundaries. As an early interventionist that goes into a family’s home, it is hard to draw a line between myself and the home I’m in. When I’m feeling overwhelmed by a family’s situation, I feel defeated and lost. She was able to lend an ear, laugh, and even let me cry when I felt in over my head. Having an MHP to guide me is essential to the support I can provide to others. —Jennilee Owens, MS, OTR/L
As a physical therapist, I am often seeing children shortly after birth when parents have had a traumatic birth experience, are dealing with medical complications surrounding birth, a diagnosis, fear of diagnosis, or loss of a “typical child.” I feel comfortable recognizing these challenges, however I am not trained in addressing needs such as post-traumatic stress, depression, and anxiety that often go along with these events. Prior to having an MHP on my team, I would refer parents to their primary care physician for guidance. Having an MHP on the EI team provides an avenue for these concerns to be explored in a timely manner as part of a multidisciplinary approach to care. Additionally, there have been many instances in my career in EI that parents have a diagnosed mental illness. This has posed challenges in interaction, communication, and family-centered treatment. Having an MHP on anEI team provides support to us as clinicians for ongoing education to better navigate these situations with families and to gain a better understanding of ways to help these families support their child’s development. —Colleen Lillis, PT, MSPT

Initial services provided by Frederick County Infants and Toddlers Program included physical therapy, occupational therapy, and infant massage. Photo: shutterstock/Onjira Leibe
While we have known for years that services must be a family approach at this age, hence, individualized FAMILY service plan, we continue to learn more about what method of intervention is most successful. It is time that we have the ability to address the family needs, which so very often starts with focusing on caregiver mental health. —Leslie Gray MOT OTR/L
When parents are not mentally present to participate in our program, less progress is made toward child outcomes. Providers tend to become frustrated when little/no progress is made, and often place blame on themselves or the families. With MHP team members who can help us identify these issues with compassion and offer ongoing support if needed, that frustration/stress is not as prevalent for me as it used to be. —Lauren Weiss MOT OTR/L
Implementing the Vision
Systemic change will be required in order to move toward increasing the presence of and expanding the role of MHPs within EI. Long overdue changes in medical assistance reimbursement policy and social work graduate-level course work will need to occur.
Medical Assistance Reimbursement
Outdated medical billing policies that are far from being trauma-informed pose one of the biggest threats to expanding mental health services to children and their families within EI in the ways described in this article. In Maryland, the Department of Health Division of Children’s Services publishes a policy and procedure manual with billing instructions for Part B and Part C services. This procedure manual severely limits the type of psychological services that a licensed mental health provider (e.g., licensed psychologist, psychiatrist, clinical social worker, or clinical counselor) can bill. Maryland medical assistance will reimburse for psychological services provided through an IFSP only if the infant or toddler is present for the session. This requirement severely limits a clinician’s ability to meet alone with a caregiver throughout the course of a child’s treatment, which is frequently clinically indicated. A flexible format that incorporates individual sessions with a parent that focus on the parent’s emotional needs is often recommended because enhanced parental well-being ultimately extends to benefit the development of the child (Lieberman & Van Horn, 2008).
FCITP is extremely fortunate in that it does not rely on medical assistance reimbursement as a primary source of program funding. Frederick County, a place where adverse childhood experiences and mental health have been a focus of local health improvement efforts for years, provides funding for a large portion of the FCITP annual budget. All of the positive programmatic changes highlighted in this article would not have been possible without this support.
Unfortunately, many jurisdictions do not have this luxury and depend on medical assistance reimbursement to fund provider positions. Allowing MHPs to bill for EI sessions where the infant or toddler is not present (in alignment with clinical recommendations and best practices) would go a long way toward improving the quality and efficacy of mental health care for these children and their families.
Social Work Curriculum
In addition to reimbursement practices, modification of graduate level curriculum to include more information about EI and the mental health and social emotional needs of infants and toddlers is another barrier that will need to be overcome in order to expand the role of the MHP within EI. Simply put, if graduate students are not exposed to a population in need, how can they ever be expected to find their way to servicing that population? Because clinical social workers are the most plentiful licensed mental health provider type, this section will focus on further analysis of their educational training.
Social workers are trained to be “generalists” who can work with all populations in countless programs and agencies, therefore graduate-level curriculum is broad. Those with a master’s of social work often take numerous courses in ethics, research, psychopathology, and substance use treatment, but may only take one or two courses targeting human development through the lifespan. Again, because this coursework covers the entire lifespan, there is virtually no exposure to infant and early childhood mental health or developmental disabilities or delays in young children. A very small percentage of clinicians who choose to specialize in clinical mental health will go on to subspecialize in infant and early childhood mental health. Matthew Melmed, executive director of ZERO TO THREE, explained, “Despite all we know about the effectiveness of early childhood mental health services, most children still do not receive necessary treatment and services. Clinicians who specialize in early childhood mental health, and particularly the needs of infants and toddlers, are scarce, limiting access to services” (2016).
Of the 300,087 clinical social workers currently employed in the United States, only 5% work in the field of education (Shao, 2021). Mental health counseling, substance use counseling, and various roles within child welfare and social services tend to be some of the most visible options for those considering a career in social work. Naturally, these agencies tend to be the most common for placing students for internships. Knowing that roughly 70% of companies offer interns a full-time job after they graduate and 80% of students accept such offers, there needs to be an improvement in making students aware of EI social work opportunities and encouragement of internship placements in this area (Zuckerman, 2020)
As a personal reflection, it is by chance that I came to work in the world of EI. As a student, I did not receive any exposure to infant and toddler mental health or EI services in my graduate course work. Following graduation, I chose a job in a community outpatient mental health clinic (the same clinic where I had completed my internship). While working in this clinic, I volunteered to serve on an interdepartmental committee with an aim to reduce adverse childhood experiences in Frederick County. The assistant program manager of FCITP also served on the committee, and it was through this connection I learned about FCITP and the role mental health clinicians can play on an EI team. Without this experience, which occurred purely by chance, I would have missed out on the opportunity to do clinical work I am vehemently passionate about simply because I was never exposed to it as an option. Sadly, I believe this is the case for far too many social work students and professionals.
Modifying current graduate level social work curriculum requirements and promoting internship placements specific to infant and early childhood mental health and Part C EI will help address what is a critical shortage of competent providers available to service this population.
Assessing Needs on a Programmatic Level
Knowing that macro change (like that mentioned in the previous section) can be quite time consuming and labor intensive, it is important to provide recommendations on a programmatic level for those wishing to move forward within their own programs or jurisdictions. Program administrators within Part C programs are encouraged to consult with other states and jurisdictions to learn more about how they can better use, or in some cases add, MHPs to the EI team. Part C program administrators are also encouraged to explore the reflective questions that follow to better assess how they are meeting the mental health and social–emotional needs of the population they serve:
- Do you have licensed MHPs (LCSW-C, LCPC, licensed psychologists) as part of your EI team? If so, how are they used (e.g., evaluation, consultation, case management, therapeutic counseling, parent training)?
- Are you screening for child trauma exposure, child mental health concerns, and child social–emotional delays at intake and evaluation? If so, do the individuals completing the screening feel they have adequate training to make a well-informed determination regarding eligibility in this area?
- What mental health needs are you noticing most frequently with the children and caregivers you work with? (e.g., anxiety, depression, substance use, grief)?
- How are you addressing the mental health needs of the population you serve?
- If you primarily rely on referrals to community resources to manage family mental and behavioral health needs, are you collecting data on successful linkage to outpatient counseling?
Author Bio
Erin Poffenberger, LCSW-C, is the systems supervisor and clinical social worker with the Frederick County Infants and Toddlers Program in Frederick, Maryland. For the past 6 years, she has been providing mental health services to children and families in outpatient clinical settings and Part C early intervention. Ms. Poffenberger has a passion for working with families of young children who are experiencing adversity and trauma and is rostered to provide several evidence-based trauma treatments including child–parent psychotherapy and trauma-focused cognitive behavioral therapy.
Suggested Citation
Poffenberger, E. (2022). Beyond case management: The role of mental health professionals within Part C Early Intervention. ZERO TO THREE Journal, 42(4), 40–61.
References
Candelaria, M., Endy, K., & Wasserman, K. (2021). Infants and Toddlers Program Infant and early childhood mental health capacity survey results (pp. 1–15) [Internal report].
Center on the Developing Child at Harvard University. (2009). Maternal depression can undermine the development of young children: Working Paper No. 8. link
Centers for Disease Control and Prevention. (2018, March 9). Individuals with disabilities education act (IDEA) services. link
Gilkerson, L., Graham, M., Harris, D., Oser, C., Clarke, J., Hairston-Fuller, T. C., & Lertora, J. (2013). Trauma-informed Part C EI: A vision, a challenge, a new reality. ZERO TO THREE Journal, 34(2), 34–44.
Lieberman, A. F., & Patricia Van Horn. (2008). Psychotherapy with infants and young children: Repairing the effects of stress and trauma on early attachment. Guilford Press.
Malone, D. M., McKinsey, P. D., Thyer, B. A., & Straka, E. (2000). Social work EI for young children with developmental disabilities. Health & Social Work, 25(3), 169–180. link. link
Masefield, S. C., Prady, S. L., Sheldon, T. A., Small, N., Jarvis, S., & Pickett, K. E. (2020). The caregiver health effects of caring for young children with developmental disabilities: A meta-analysis. Maternal and Child Health Journal, 24(5), 561–574. link. link
Melmed, M. (2016, July 13). Effective mental health treatment for young children and their families. HuffPost. link link
National Academies of Sciences, Engineering, and Medicine; Division of Behavioral and Social Sciences and Education; Board on Children, Youth, and Families; Committee on Supporting the Parents of Young Children; Gadsden, V. L., Ford, M., & Breiner, H. (Eds.). (2016). Parenting matters: Supporting parents of children ages 0–8. National Academies Press.
Shao, H. (2021, December 14). Clinical social worker demographics and statistics [2022]: Number of clinical social workers in the US. link
Thomson, K. C., Jenkins, E., Gill, R., Richardson, C. G., Gagné Petteni, M., McAuliffe, C., & Gadermann, A. M. (2021). Impacts of the COVID-19 pandemic on family mental health in Canada: Findings from a multi-round cross-sectional study. International Journal of Environmental Research and Public Health, 18(22), 12080. link. link
Woodman, A. C., Mawdsley, H. P., & Hauser-Cram, P. (2015). Parenting stress and child behavior problems within families of children with developmental disabilities: Transactional relations across 15 years. Research in Developmental Disabilities, 36, 264–276. link link
Young, N. K., Gardner, S., Otero, C., Dennis, K., Chang, R., Earle, K., & Amatetti, S. (2009). Substance-exposed infants: State responses to the problem. HHS Pub. No. (SMA) 09-4369. Substance Abuse and Mental Health Services Administration.
Zuckerman, A. (2020, May 26). 98 internship statistics: 2020/2021 data, trends & predictions. CompareCamp.Com. link