Lee Hinton, Saskatchewan Prevention Institute, Saskatoon, Saskatchewan, Canada
Nana Esi Gaisie, Effia Nkwanta Regional Hospital, Sekondi, Ghana
Kerrie L. Schnake, South Carolina Program for Infant/Toddler Care, Charleston, South Carolina
Ekaterina Zoubak, Substance Abuse and Mental Health Services Administration, Rockville, Maryland
Abstract
Adaptive leadership requires that practitioners push the boundaries of current policies and systems to provide optimal services to children and families. This process includes self-reflection, strategic positioning, building relationships with advocates, inspiring service providers and policymakers, and creating a shared vision. This article explores the use of adaptive leadership to move systems and policies forward in a hospital setting in Ghana, provincial and community-based work in Canada, and through infant and early childhood mental health networks. Building relationships and empowering leaders to advocate both independently and as part of a group can help leverage the influence needed for change.
System and policy change do not take place in a vacuum. One individual or organization cannot bring about change. Instead, change requires collaboration, inspiration, persistence, and motivation. Successful change leaders have strengths in the areas of communication, leading collaborative efforts, initiating the change process, helping to develop a shared vision of change, strategizing a path forward, and motivating others to commit to the process of change no matter how long it takes (Centre for Creative Leadership, 2019). Adaptive leaders, armed with these qualities, have the capacity to change systems and inform policies that can ultimately promote the well-being of young children and their families.
Leadership Skills in Promoting Systems and Policy Change
This article examines five key leadership areas—collective strategies, the role of inspiration, seeing the bigger picture, working from a place of change, and accepting the vulnerability of change necessary for effecting change in early childhood mental health systems and policies. In addition, three case examples highlight these concepts along with reflection on the successes and challenges when working to evoke change at higher levels of administration. Ultimately, successful leaders have a responsibility to promote and maintain systems that provide both access and equitable and inclusive opportunities for all.
Collective Strategies
Developing collective strategies for system and policy change is crucial and should involve stakeholders from a variety of sectors; both allies and unlikely allies (Heifetz, Grashow, & Linsky, 2009). Collective strategies require leadership to establish a common goal, foster trust amongst stakeholders, and facilitate flexibility and diverse perspectives (Reeves & Bernhardt, 2013). Such leadership values diverse views, persistence, and disequilibrium (Heifetz et al., 2009). Together, collective strategies and leadership that reflects diverse voices are more coordinated in reaching a common goal for change.
The Role of Inspiration
Adaptable leadership for system and policy change requires the ability to inspire others as others must see in themselves the same desire for change if there is to be any movement. Inspiring others starts from an inquiry of why; instead of how and what (Sinek, 2009). Why does there need to be change? Why should people care enough to work together? Inspiration and motivation results in a shared vision and leads to action (Sinek, 2009).
Seeing the Bigger Picture
Using tools related to systems theory can help stakeholders to see the bigger picture. From this view, strategies for change can be developed that are long-term, sustainable, and impactful. Seeing the bigger picture helps stakeholders to see the ways that they are connected to one another, improves their relationships, and increases accountability (Stroh, 2015). Seeing the bigger picture also empowers stakeholders to look beyond current crisis and ongoing trends and patterns and consider the root causes of events. It is important to look at how these positive and negative causes shape, drive, and stabilize the current system. Doing so can also help to determine how resistant the system will be to change (Stroh, 2015).
To prepare leaders for longer-term expansive plans, Argyris’ and Senge’s Ladder of Inference provides a tool that helps leaders, groups of stakeholders, or both, slow down, avoid jumping to conclusions and quick-fix solutions, and base plans on facts and long term-goals (Argyris, 2012; Mind Tools, 2018; Mulder, 2018; Senge, 2014; Senge, Hamilton, & Kania, 2015).
Working From a Place of Change
Adaptive leadership is best in unpredictable environments that persistently change. Change requires flexible goals, tactics, and resources (Heifetz et al., 2009). As such, leadership can help shape this unpredictable environment; using innovation to move causes forward (Reeves, Deilmer, Love, & Timmanns, 2013).
When strategically considering collective action in the area of system and policy change, it is important to be aware that some factors within the environment are unpredictable and constantly changing. It is important to understand what factors are malleable and the extent that those involved can influence these (Deimler, Lesser, Rhodes, & Sinha, 2013). Adaptive leadership skills allow practitioners to look beyond short-term reactive problem solving to focus on long-term solutions created by innovation and change (Senge et al., 2015), thus creating a match between a changing environment and adaptive skills to meet those changes.
Accepting the Vulnerability of Change
When striving and advocating for systems and policy change, it is important to examine how the current systems and policies have come into being. Each stakeholder involved benefits in some way from the current system. Without identifying how the current system advances those at the table, leaders who are seeking change will struggle against those who wish to maintain the status quo. After all, the status quo is safe and does not lead to loss (Heifetz et al, 2009; Stroh, 2015).
Change requires courage. This courage can be found within relationships built through adaptive leadership. The courageous tasks of collective action include taking time and not rushing into short-term solutions, working across sectors that do not normally work together, creating disequilibrium and taking risks, being willing to risk failures, and looking at the situation from an objective view (Heifetz et al., 2009; Reeves & Deilmer, 2013; Stroh, 2015).
Examples in the Field
The following case studies highlight the use of adaptive leadership and collective action to benefit very young children. Each case presents different contexts–local and international— and varying infant and early childhood mental health (IECMH) priorities that are being elevated through a lens of systems and policy change.

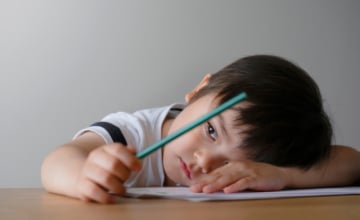
The current landscape of child- and family-serving sectors will need to be disrupted and re-envisioned to make room for new ways of thinking. Photo: Studio1One/Bigstock
Saskatchewan, Canada: Increasing Systems Capacity to Address Early Childhood Mental Health Knowledge
Within the province of Saskatchewan, funding for infants and toddlers is often granted to targeted, intervention programming focused on children and families who fall into mandated risk categories. Many do not fall into this catchment criterion in the early years, because risk may not be determined until the child is older. As a result, many families do not receive support to enhance their child’s development and mental health despite the fact that it has been well-established that the formative years provide a strong foundation for later physical and mental health.
In response to this gap, the Saskatchewan Prevention Institute has taken a leadership role within the province to establish an IECMH program. This program focuses on promoting and supporting early childhood mental health through knowledge exchange and translation of evidence-based information, networking, building community capacity, educating and building capacity with parents, sharing promising and innovative practices, and advocating for systemic change. Taking a multi-sectoral, strength-based approach, the program focuses on the prevention of poor mental and physical health, and it supports strategies that enhance brain development, nutrition, attachment, resilience, play and exploration, responses to trauma, and emotional regulation.
Part of this leadership role and community capacity building led to the development of the Saskatchewan Early Childhood Mental Health Network, the La Ronge Tri-Area Early Childhood Mental Health Network, Research and Development Communities of Practice, and the Early Childhood Educators Early Childhood Mental Health Network (ECE-ECMHN). These groups bring together provincial and national multi-sectoral professionals to share new research and promising, innovative practices, participate in professional development opportunities, advocate for system change, and work together on collaborative projects.
Child care providers have the opportunity to model, support, and educate parents about early childhood mental health and development; including strategies that can help children grow optimally (Gold, 2017; Lieberman, 2018; Schein, 2018). In Saskatchewan, both licensed and unlicensed child care options are available to parents. Licensed child care services are accredited and monitored through the Government of Saskatchewan, Ministry of Education. Of Saskatchewan children whose families need child care services, 70% cannot access licensed child care due to a lack of availability in their communities and limited space in centers (Carlberg & Budney, 2019; Macdonald, 2018). These families often use unlicensed child care services (Carlberg & Budney, 2019; Macdonald, 2018). Unlicensed child care is not monitored, but providers are required to meet the child–caregiver ratio set by the Child Care Regulation 2015 (Government of Saskatchewan, 2015).
Providing support to child care professionals should include specialized professional development opportunities focused on early child development and mental health. Although some basic training is often required for those working in licensed child care facilities, the topic and type of professional development is often the choice of the professional, and attending traditional, in-person opportunities may be unrealistic due to staff coverage issues. Those working in unlicensed child care facilities have differing levels of experience and education, and often do not have access to the same training opportunities as those who work in licensed homes or centers. As well, early childhood professionals often do not get support to integrate information into practice due to a lack of time to reflect on and introduce new strategies into practice (Arjona, 2011; Bromer & Bibbs, 2011; McCabe et al., 2011).
In recognition of the gap in appropriate and accessible professional development for child care workers, the ECE-ECMHN put forward a set of recommendations that included: developing online open education modules, continuing to engage professionals through the network, and advocating for the inclusion of early childhood mental health modules through training programs. This same group will help develop, disseminate, and review learning modules to ensure that they meet the needs of their colleagues. For the Saskatchewan Prevention Institute, a collaborative approach to system change adds strength as each perspective is weighed and considered while the group comes to a united approach to effecting change.
South Carolina, United States: Building Strong Networks
In many states throughout the US, efforts related to early childhood mental health are still in their infancy. Adaptive leadership strategies are effective in guiding the intentional growth of IECMH systems. These strategies are particularly useful in instances where this work is just beginning to take root and therefore brings with it new and unfamiliar terminology, philosophy, and approaches. The current landscape of child- and family-serving sectors will need to be disrupted and re-envisioned to make room for new ways of thinking, changes in policies, and relationship-centered practices. While the systemic tide is only just beginning to shift in support of very young children and families’ mental health, the work done so far toward this effort in South Carolina represents an adaptive leadership approach.
To ensure dedicated attention to the issue of building the state’s capacity to support IECMH, the South Carolina Infant Mental Health Association (SCIMHA) was established. The multidisciplinary nature of IEMCH makes coordinated leadership particularly critical. Adaptive leadership requires that leaders hold multiple perspectives in mind when guiding change. In order to achieve a vision for change, leaders must take time to look at the big picture. SCIMHA is guided by leaders from multiple child-serving disciplines and provides space to view goals in the context of the larger coordinated vision for IECMH in the state. These diverse perspectives help ensure that services for young children and their families are considered holistically. IECMH has a home across and within all child- and family-serving sectors, whether the work is addressing promotion, prevention, or treatment. SCIMHA provides a common, strength-based, relationship-oriented lens from which all service providers can orient their work, which provides consistency for families who may be engaged with more than one service entity.
With SCIMHA established and engaging child- and family-serving professionals from many disciplines, the state was ready to join more than half of the states in the country in licensing the IECMH Workforce Competencies and Endorsement® from the Alliance for the Advancement of Infant Mental Health. Funding from the South Carolina Department of Social Services, Division of Early Care and Education supported SCIMHA in licensing the Endorsement® to create a concrete and tangible framework on which the group could mobilize efforts to support IECMH.
Not long after the adoption of the IECMH Competencies, SCIMHA, acting jointly with stakeholders from the state’s Medicaid agency, child welfare agency, mental health agency, early care and education sector, and higher education institutions, submitted an application for technical assistance from ZERO TO THREE which coalesced the engagement of key child- and family-serving partners. The opportunity provided by ZERO TO THREE helped set the stage for adaptive growth by inspiring key stakeholders to undertake the exploration and discovery of the state’s IECMH landscape with an objective lens. This collaborative experience created a climate for embracing opportunities for growth and acknowledging gaps with a commitment to change rather than admonishing deficiencies.
In South Carolina, the large gaps in available services and professional expertise needed to support the social–emotional health of very young children was somewhat hidden under the mission statements of many of the state’s organizations, agencies, coalitions, and institutions proclaiming to focus on children from birth to older ages. While the intent is clearly to support children from the time of birth, adequate and appropriate specialized workforce training to support the intent has not been a priority in all child-serving institutions. Using adaptive leadership strategies including knowledge building through stories and education, a focus on relationship building, and a commitment to change, key child- and family-serving representatives worked together to uncover the gap between the intent of their organizations and the reality of services provided. The task of discovery was taken on with humility and a sincere desire to understand the status of babies in the state. The task was also motivated and inspired by exposure to information that created a new understanding of the incredible opportunities and vulnerabilities that occur within the first 3 years of life.
Inspiration for action can be achieved in many ways. In this instance it was a South Carolina team of stakeholders traveling to participate in a 2-day ZERO TO THREE Infant and Early Childhood Mental Health Finance and Policy meeting with other state teams. Adaptive leadership requires flexible goals, tactics, and resources. A skilled leader must recognize which resources can help achieve the desired vision for change and when best to use them.
Meanwhile, IECMH champions supported by SCIMHA were regularly presenting at meetings and conferences where stakeholders and potential partners were in attendance. This outreach resulted in relationships with advocates across sectors including agencies and organizations responsible for direct service to infants and their families as well as agencies serving adolescent and adult populations for whom interventions during infancy may have eliminated the need for later services.
As the work has progressed in South Carolina, leading IECMH change agents have not been impervious to the vulnerability that comes with change. Promoting a vision with new ideas that challenge the status quo, even when the new ideas are favored, will create tension. As priorities, attention, and investments shift, the leaders driving the change will no doubt feel the sting of those who are benefiting from the current system and who are unwilling or unable to envision a future that diverges from the status quo. The ability to navigate such tensions lies in the assurance that comes from the support garnered in a collective approach to change that is driven by an inspired vision. Each committed stakeholder will, to the extent possible within their context, disrupt the status quo in favor of change that supports babies and families.
Ultimately, when an inspired vision for change has taken root and is moving forward using a collective strategy for adaptive change, many will contribute significantly to the effort, some will contribute minimally to the effort, and a small number will actively work to stymie change. An adaptive leadership approach will ensure a vision for change that (a) the collective partners have agreed upon, (b) drives decisions that leverage the strengths of current systems, and © builds resources and knowledge where needed.

Although Ghana was one of the first countries to ratify the United Nations Convention on the Rights of the Child in 1990, it has struggled to fulfill its mandate of seeking the best interest of all Ghanaian children. Photo: Nana Esi Gaisie
Ghana, West Africa: From Practice to Policy
Although Ghana was one of the first countries to ratify the United Nations Convention on the Rights of the Child in 1990, it has struggled to fulfill its mandate of seeking the best interest of all Ghanaian children. Children with special needs or those in orphanages or on the streets have been largely ignored and remain at risk. Even though human rights watchers and child advocates have continually expressed the need to come to the aid of such children and help unearth their potentials, it was a task seen to be Herculean by those responsible for their well-being.
Certain beliefs, cultural underpinnings, and the understanding of young children has shaped the approach and value placed on infants, children, and young adults in Ghana. Children born with disabilities were thought to be abominable, resulting in continued rejection and suffering due to the persistent stigma. In addition, the primary focus for years of all maternal and child health programs has been the survival of the child. The Millennium Development Goals challenged Ghana to improve mortality and morbidity rates at a time that the whole world had moved into another conversation of improving the quality of lives of children beyond survival.
As Ghana, like other developing countries, was struggling to prevent neonatal and early childhood deaths, a discussion about quality of life was premature. It was not surprising, then, that policymakers did not have much to say about the promotion of IECMH in Ghana’s Under Five’s Child Health Policy: 2007–2015. This policy stated:
Physical and mental disabilities do not contribute significantly to overall child mortality and morbidity. It is recognised that more data on the epidemiology of physical and mental disabilities in young children are needed. The child health program will advocate for collection and use of appropriate data in planning interventions to address these. A number of interventions or strategies that are currently a part of the child health program will prevent some childhood disabilities, including: pregnancy interventions, polio vaccinations, measles vaccination, Hib vaccination. Improvement of the nutritional status of children, including micronutrients such as iodine, may improve long term cognitive status. Strategies to prevent and manage violence and abuse against children and to manage orphans may help to prevent the long term sequelae of abuse or neglect. The management of children with existing long term mental and physical disabilities from congenital malformations, birth trauma and other factors needs improvement. More data are needed on the extent of these problems, and on the most cost effective approaches to managing them. (Ministry of Health, Ghana, 2007, p. 19)
Clearly troubled by the seeming neglect and indifference toward the plight of such children, a group of Ghanaian teenagers decided to challenge the system even before this policy was born. These brave teenagers came together to serve the needs of such children, not only as a social responsibility, but also as a way of highlighting that young children with special needs also had something meaningful to contribute to society if given the right support. The work of this young group set aside childhood ambitions and began with advocacy against strong institutions.
The first strategy was to build capacity in knowledge and skills in order to speak and advocate from an informed position. Some went on to study medicine while others went on to study psychology. This was a collective strategy, which was supported by prominent adults who believed their intent was noble. They were met with resistance, even from their parents, as some had to convince stakeholders for support in these initiatives. After a decade of quiet commitment by way of building capacity toward this long-term goal, the advocates started to coordinate further, feeling more inspired and courageous to make the needed changes in this matter. The dream for supporting at-risk children with needs had never died. Instead, it was emboldened by the ongoing reports in the newspapers of children being abused, of children being trafficked abroad, and of institutionalized orphans being abused.
Associating with lecturers in the University of Haifa further exposed this group to research about child development, aligning well with the demands for research noted in Ghana’s short-sighted Under Five’s Child Health Policy 2007–2015. The training and access to data on child outcomes provided a firmer understanding of the interconnection between research, policy, and practice, and that these things are actually bedfellows. Moreover, the group looked for opportunities to be heard back in Ghana where they sought opportunities to speak on TV and radio about the value of children, developmental milestones, nutrition-specific and nutrition-sensitive interventions for children, and other topics. The TV program known as Fruit of the Womb was one of such educational initiatives. (Opoku, 2017).
In these efforts to learn and disseminate information on the importance of early development for all young children, these Ghanaian advocates recognized that parents, families, and caregivers were well-meaning and were parenting based on the limited information they were receiving. This knowledge only highlighted the need to create massive awareness, and print and social media were not to be left out as avenues of communication. Such efforts ensured that parenting was grounded in firm knowledge of the developmental needs of children, promoting a decrease in potential parenting strategies that could do harm. In this spirit, events such as World Prematurity Day and World Autism Day were used as a platform to disseminate and promote knowledge. Specific efforts ensured that the community would hear the importance of the early years and that this was the best time to identify and intervene in abnormal development because of brain development, plasticity, and the science behind it.
Also, the group spearheaded efforts to remove harmful primary education literature that promoted cultural stereotypes that helped maintain the status quo in undermining the value of early brain development and opportunities for young children in Ghana. One particularly damaging sterotype stated that the brain was used simply to carry loads of goods and supplies. The national debate ultimately resulted in the textbook being removed from schools and efforts to educate the public and share research on the value of the brain that was rooted in science. (Ghanaweb, 2016)
The advocates have worked tirelessly to educate the public on the importance of the early years at each opportunity— including during hospital trainings on newborn care, during clinical meetings, during Nestle nutrition seminars, and during child protection conferences. At the same time, the group realized that leveraging change at a national systems level required advocacy at the policy level. The years of grassroots efforts and exposure that were used to scaffold their learning and effectiveness as advocates resulted in their efforts being showcased at the Survive and Thrive Conference in July 2019 held by the Ghana Health Service in collaboration with the World Health Organization, the United Nations Children’s Fund (UNICEF), and other partners. This conference saw the birth of a new child policy that sought to introduce the integration of the Nurturing Care Framework and Early Childhood Development in Paediatric care; a policy that garnered a great deal of excitement in the community because of the years of committed conversation around its need for vulnerable children in Ghana. The advocates had in large part laid the foundation for a seamless acceptance and embracing of this new system/policy and way of thinking about supporting early development that emphasized the best interest of the child.

Bettering the lives of very young children requires adaptive leaders and a deep understanding that larger systemic and policy changes require a long-term commitment, collaboration, and leading through consensus. Photo: Rob Hainer/shutterstock
The Ghana National Newborn Health Strategy and Action Plan: 2019–2023 (Ministry of Health, Ghana, 2019, p. 22) was born from these events and states under the subject “Follow-up care to support the Survive and Thrive approach:”
- Initiation of activities addressing psychosocial support for mothers/families who have undergone adverse events such as the loss of a baby, etc
- Promotion of early childhood development to be addressed through the implementation of the UNICEF/ World Health Organization Nurturing Care Framework launched in June 2018.
This policy was a major milestone in codifying the importance of psychosocial supports to families and recognition of development for all children including those with special needs. This general statement also set the stage to pilot interventions in this field successfully for national use. Two major areas include examining the ways in which psychosocial support can be offered effectively to parents/families of children with special needs and integrating early childhood development and developmental screening into routine pediatric care. In addition, the Mental Health Authority in Ghana has provided an invitation to draft policy on IECMH for the nation in recognition of their proactiveness in the field.
There is a need for Ghana to establish clearly defined policies for early identification of common disabilities and impairments among Ghanaian children from birth to 5 years old with corresponding interventions, while fighting marginalization and stigma. To successfully achieve this, many of the key leadership strategies have been applied including collective action in accepting the vulnerability of change that requires courage to approaching leading institutions and authorities that can make a difference for all children in Ghana. These skills were gained in part from the ZERO TO THREE Fellowship. This work has only highlighted additional opportunities for growth including improving the workforce and building a multi-professional system for care for children with special needs. Ghana, in this case, provides an excellent example of impact when the focus elevates experiences of frontline advocates and leaders within communities to the policy level.
Conclusion
Fostering change in the status quo, or the equilibrium state, of a system, can take many forms. The jumping off point and access to a solid infrastructure that helps to propel these efforts forward vary greatly from state to state, province to province, and from country to country. In all cases, however, an inspired vision and the ability to lead while being flexible to accommodate unanticipated challenges and alternate opinions are necessary.
The three case studies in this article offer brief snapshots into global efforts that create a better functioning and more equitable set of supports for the youngest, and most vulnerable, children. These examples seek to inspire readers to engage in addressing multilayered, adaptive challenges. Bettering the lives of very young children requires adaptive leaders and a deep understanding that larger systemic and policy changes requires long-term commitment, collaboration, and leading through consensus. With inspired effort and commitment to increase equity and inclusion in systems and policies serving the most at-risk children, such visions and long-term plans lay the foundation for sustainable system growth and improvement for generations to come.
Disclaimer
This article was co-authored by Ekaterina Zoubak in her personal capacity. The opinions expressed in this article are the author’s own and do not reflect the official views of the Substance Abuse and Mental Health Services Administration, the Department of Health and Human Services, or the United States government.
Author Bios
Lee Hinton, MSW, is program manager at the Saskatchewan Prevention Institute. Ms. Hinton’s career has focused on children’s, women’s, and family health and well-being. She obtained her undergraduate degree from the University of Waterloo, holds a postgraduate degree in art therapy from the University of Western Ontario, and a master’s of social work from Wilfred Laurier University. Ms. Hinton is a member of the 2018–2020 ZERO TO THREE Fellowship Class. She has worked at a variety of organizations focused on health and well-being, including the London Regional Cancer Centre, Region of Peel (Ontario); Sexual Assault Centre of London; Women’s Mental Health/Addictions Action and Research Coalition; and YWCA Saskatoon; and is on several national and provincial boards and advisory committees that are focused on early childhood mental health. Ms. Hinton has been the program manager at the Saskatchewan Prevention Institute since 2007. She works with communities throughout Saskatchewan and participates on national and provincial projects and advisory committees to develop a common knowledge-base and increase agreement regarding the importance of the early years. Ms. Hinton developed and coordinates the Early Childhood Mental Health Program, which focuses on bringing emerging, evidence-based information and training to professionals throughout the province.
Nana Esi Gaisie, MBChB, MA, is a pediatric staff physician at Effia Nkwanta Regional Hospital, the regional hospital in the Western region of Ghana. Dr. Gaisie’s aspiration is to promote the best interest of every child, especially children with special needs, in their survival, development, protection, and participation. This is her motivation for setting up a nonprofit organization at 18 years old and for authoring a book on marriage to support spousal relationships. She has since followed this passion for 2 decades. She holds a bachelor’s degree in human biology, bachelor of medicine and bachelor of surgery degree from the Kwame Nkrumah University of Science and Technology in Ghana, and a master’s degree (cum laude) in international child development in developing countries from the University of Haifa, Israel. She is currently a ZERO TO THREE Fellow, and has recently been tasked by the Mental Health Authority in Ghana to draft a national policy for infant and early childhood mental health. Dr. Gaisie is the recipient of a 2015 award from University of Haifa for outstanding project work in the International Masters in Child Development in Developing Countries program and for the best poster presentation at the 2019 joint World Health Organization (WHO) and Ghana Health Service Newborn stakeholders’ conference.
Kerrie L. Schnake, MA, is the director of the South Carolina Program for Infant/Toddler Care, South Carolina’s Infant/ Toddler Specialist Network, which she established in 2006 for the South Carolina Department of Social Services, Division of Early Care and Education. She is also the founder of the South Carolina Infant Mental Health Association. Prior to moving to South Carolina, Ms.Schnake worked in California at WestEd’s Program for Infant/Toddler Care and as a research assistant at the WestEd Center for Child and Family Studies. Ms. Schnake is a leader in South Carolina’s work to promote the social– emotional health of the very young. She holds a bachelor’s degree in sociology from Cal State, East Bay, and a master’s degree in early childhood education with an emphasis in public administration from San Francisco State University. She is a member of the 2018–2020 ZERO TO THREE Fellowship Class.
Ekaterina Zoubak, MA, is a public health advisor with the Substance Abuse and Mental Health Services Administration (SAMHSA), U.S. Department of Health and Human Services. Ms. Zoubak currently serves as a federal project officer for Project LAUNCH (Linking Action for Unmet Needs in Children’s Health), the Infant and Early Childhood Mental Health, and Mental Health Awareness Training grant programs. In this capacity, she works closely with states, territories, tribal organizations and governments, and a variety of other organizations and entities to advance infant and early childhood mental health and maternal mental health efforts. She is the lead for projects related to American Indian and Alaska Native communities within the Project LAUNCH program and the coordinator for Indigenous Project LAUNCH. Ms. Zoubak has been involved in various cross-agency federal initiatives and efforts focused on early childhood and children’s mental health. Prior to joining SAMHSA, she provided group and individual mental health services to children and adolescents within schools and psychiatric settings. She holds a bachelor’s degree in psychology and a master’s degree in clinical psychology. She is a member of the 2018–2020 ZERO TO THREE Fellowship Class.
Suggested Citation
Hinton, L., Giasie, N. E., Schnake, K. L., & Zoubak, E. (2020). Cultivating adaptive leaders to drive system and policy change. ZERO TO THREE Journal, 40(5), 12–19.
References
Arjona, B. (2011). Voices from the field: Family child care providers in their own words. ZERO TO THREE Journal, 31(5), 62–63.
Argyris, C. (2012). Organizational traps: Leadership, culture, organizational design. London, UK: Oxford University Press.
Bromer, J., & Bibbs, T. (2011). Improving support services for family child care through relationship-based training. ZERO TO THREE Journal, 31(5), 30–37.
Carlberg, C., & Budney, J. (2019). Saskatchewan’s failing report card on child care. Retrieved from source
Center for Creative Leadership. (2019). How to be a successful change leader. Retrieved from source
Deimler, M., Lesser, R., Rhodes, D., & Sinha, J. (2013). Own the future: 50 ways to win from The Boston Consulting Group. Hoboken, NJ: John Wiley & Sons.
Ghanaweb. (2016). Prof-Quarm’s textbook not approved for schools – Edu. Ministry. Retrieved from source
Gold, C. (2017). The developmental science of early childhood: Clinical applications of infant mental health concepts from infancy through adolescence. New York, NY: W.W. Norton and Company.
Government of Saskatchewan. (2015). The child care regulations, 2015. Regina, SK: Government of Saskatchewan: Government Publications.
Heifetz, R., Grashow, A., & Linsky, M. (2009). The practice of adaptive leadership. Tools and actions for changing your organization and the world. Boston, MA: Harvard University Press.
Lieberman, A. (2018). The emotional life of the toddler. New York, NY: Simon & Schuster.
Macdonald, D. (2018). Child care deserts in Canada. Retrieved from <ahref=https: www.="" policyalternatives.ca="" publications="" reports="" child-care-deserts-canada="">source</ahref=https:>
McCabe, L., Peterson, S., Baker, A., Dumka, M., Brach, M., & Webb, D. (2011). Lessons learned from home visiting with home-based child care providers. ZERO TO THREE Journal, 31(5), 22–29.
Mind Tools. (2018). The ladder of inference. How to avoid jumping to conclusions. Retrieved from source
Ministry of Health, Ghana. (2007). Under five’s child health policy 2007-2015. Retrieved from source
Ministry of Health, Ghana. (2019). Ghana national newborn health strategy and action plan 2019-2023. Accra: Ghana Publishing Company.
Mulder, P. (2018). Ladder of influence. Retrieved from source
Opoku, I. (2017). Fruit of the Womb trailer. Retrieved from source
Reeves, M., & Berhardt, A. (2013). Systems advantage. In M. Deimler, R. Lesser, D. Rhodes, & J., Sinha (Eds). Own the future: 50 ways to win from The Boston Consulting Group (pp. 27–33). Hoboken, NJ: John Wiley & Sons.
Reeves, M., & Deilmer, M. (2013). Adaptability: The new competitive edge. In M. Deimler, R. Lesser, D., Rhodes, & J., Sinha (Eds). Own the future: 50 ways to win from The Boston Consulting Group (pp. 19–26). Hoboken, NJ: John Wiley & Sons.
Reeves, M., Deilmer, M., Love, C., & Timmanns, P. (2013). Why strategy needs a strategy. In M. Deimler, R. Lesser, D., Rhodes, & J., Sinha (Eds). Own the future: 50 ways to win from The Boston Consulting Group (pp. 11–18). Hoboken, NJ: John Wiley & Sons.
Schein, D. (2018). Inspiring wonder, awe, and empathy: Spiritual development in young children. St. Paul, MD: Red Leaf Press.
Senge, P. (2014). The fifth discipline fieldbook: Strategies and tools for building a learning organization. New York, NY: Doubleday.
Senge, P., Hamilton, H., & Kania, J. (2015). The dawn of systems leadership. Retrieved from Standford Social Innovation Review. source
Sinek, S. (2009). Start with why. How great leaders inspire everyone to take action. New York, NY: Penguin Group.
Stroh, D. (2015). Systems thinking for social change: A practical guide to solving complex problems, avoiding unintended consequences, and achieving lasting results. White River Junction, VT: Chelsea Green Publishing.