Julie Cohen and Paola Andujar, ZERO TO THREE Policy Center, Washington, DC
Abstract
States need a policy and systems infrastructure that creates a robust continuum of mental health supports and services for infants, young children, and families. One critical element of this continuum is developmentally appropriate diagnosis. DC:0–5TM: Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood (DC:0–5) is a system for classification of mental health and developmental disorders of infants and young children and is the recommended practice for the clinical conceptualization and diagnosis of children (birth through 5 years old). Over the past 5 years, states have pursued a variety of strategies to integrate DC:0–5 in state policy and systems.
Infants and young children can have mental health and developmental disorders that affect development. When a young child has a mental health disorder, it is important to identify and treat the disorder as early as possible so that impairment, suffering, and effects on overall health and development can be reduced. States need a policy and systems infrastructure that creates a robust continuum of supports and services for infants and young children. The ideal continuum includes supports addressing promotion, prevention, assessment, diagnosis, and treatment. One critical element of the continuum is developmentally appropriate diagnosis. DC:0–5TM: Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood (DC:0–5; ZERO TO THREE, 2016) is a system for classification of mental health and developmental disorders of infants and young children (see Box 1) and is the recommended practice for the clinical conceptualization and diagnosis of children (birth through 5 years old). Adopting DC:0–5 as a standard of practice can be an effective strategy for improving access to infant and early childhood mental health (IECMH) services and supports and improving outcomes for infants and young children. This is an area where states have been innovating since DC:0–5 was published in December 2016.
Box 1: What Is DC:0–5?
DC:0–5TM: Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood (DC:0–5) was created to provide developmentally specific diagnostic criteria and information about mental health disorders in infants and young children. The American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM, 2013) and World Health Organization’s International Classification of Diseases (ICD, 1992) are comparable classification systems for older children, adolescents, and adults. DC:0–5, published in December 2016, revised and updated Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood: Revised Edition (DC:0–3R) by expanding the age range from 3 years old through 5 years old, extending criteria to younger ages, and including all disorders relevant for young children.
This article highlights how DC:0–5 can support IECMH, discusses why and how states are integrating DC:0–5 into state policy and systems, and shares three state stories to capture some of the strategies that states have used over the past 5 years. It is important to note that this article provides a point-in-time overview. The state stories included are just a sample of the groundbreaking work going on across the United States.
How Can DC:0–5 Support IECMH?
IECMH manifests in relationships. The social–emotional health of infants and young children is closely intertwined with that of their parents and other caregivers. Mental health problems often present much differently in early childhood than in later childhood and adulthood. Existing classification systems, such as the Diagnostic and Statistical Manual of Mental Disorders (DSM-5, 2013) and International Classification of Diseases (ICD; World Health Organization, 1992), are geared toward disorders in school-age children, adolescents, and adults, and do not adequately reflect relationship-based mental health issues that are typically first diagnosed in infancy and early childhood. DC:0–5 provides empirically based, developmentally appropriate criteria to determine clinical disorder. Assessing the relationship between a child and caregiver helps to determine whether there is a need for changes or support in strengthening the caregiver–child relationship. DC:0–5 is used and recognized as the system for diagnosing mental health and developmental disorders in infants and young children within their caregiving relationship.
DC:0–5 also provides a common language that allows individuals across disciplines—including mental health clinicians, counselors, physicians, nurses, early interventionists, social workers, and researchers—to communicate accurately and efficiently with each other. An accurate diagnosis using DC:0–5 guides treatment for the child, may indicate services needed for the family, and can help determine the need for additional supports. It also allows clinicians and researchers to link knowledge about IECMH disorders to treatment approaches and outcomes. Finally, a DC:0-5 diagnosis may serve to authorize treatment and reimbursement.
State Strategies
Over the past 5 years, states have pursued a variety of strategies to integrate DC:0–5 in state policy and systems. For example, some states are allowing, promoting, or even requiring that mental health clinicians use DC:0–5 for IECMH diagnoses to receive reimbursement. A few states are exploring incorporation of DC:0–5 into electronic health record (EHR) systems so they can (a) record and track DC:0–5 diagnoses and (b) track treatment for specific diagnoses of infants and young children. Other states are using DC:0–5 in cross-sector workforce development efforts to build workforce capacity and promote widespread use of DC:0–5. The three state stories that follow provide a glimpse into the journeys of IECMH champions in Washington, Nevada, and Massachusetts, as they took on the challenge of making DC:0–5 a part of their child-serving systems. Each of the states focused on a distinct aspect of policy and systems building, using their creativity and dedication to make significant change for infants, young children, and their families.
State Policy Story: Washington
States are starting to recognize and require DC:0–5 disorders as eligible behavioral health conditions for children under 5 years old. Infants and young children manifest mental health challenges in different ways than older children. Several states have explicitly called for the use of DC:0–5 in state policy. Washington passed legislation in 2021 requiring providers to use DC:0–5 for the assessment and diagnosis of children from birth to 5 years old. Minnesota served as a model for Washington in developing the language and package.
The Innovation
Washington passed legislation in April 2021 requiring providers to use DC:0–5 for assessment and diagnosis of children from birth through 5 years old. The legislation also allows for reimbursement for up to five sessions for purposes of intake and assessment and allows for reimbursement for provider travel so assessments can be done in the home or in community settings. While not written into the legislation, accompanying proviso funds include monies to provide training for mental health clinicians who are diagnosing and allied professionals who are part of that system of care. There is also money to fund a Washington State Health Care Authority (HCA) full-time employee to support implementation of this policy, including the development of a crosswalk between DC:0–5 and ICD-10.
The Impetus
During the 2015–2016 legislature, the state of Washington passed House Bill (HB) 2439: Increasing Access to Adequate and Appropriate Mental Health Services for Children and Youth. HB2439 was a landmark bill for the state, as it established the Children’s Mental Health Work Group (renamed the Children and Youth Behavioral Health Work Group, CYBHWG) to identify and address barriers to access for behavioral health services for children, youth, and families, and make recommendations to the legislature on statewide mental health services for this population, with a particular focus on children birth to 5 years old. Members of the workgroup include legislators, providers, agencies, managed care organizations, tribes, parents, pediatricians, and other stakeholders. Specifically, the bill required that the CYBHWG review and recommend developmentally, culturally, and linguistically appropriate assessment tools and diagnostic approaches that managed care plans and behavioral health organizations should use as the mechanism to establish eligibility for services, with a focus on birth to 5.

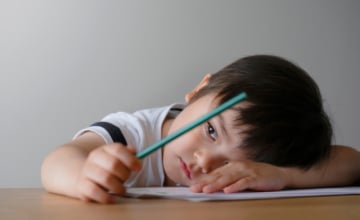
When a young child has a mental health disorder, it is important to identify and treat the disorder as early as possible so that impairment, suffering, and effects on overall health and development can be reduced. Photo: shutterstock/Zoran Zeremski
The Process
In December 2016, CYBHWG submitted their recommendations report to the legislature, including a requirement that HCA assemble a work group to identify standardized mental health assessment, outcome, and diagnostic tools (culturally and developmentally appropriate for children birth to 5) that support access to services.
In 2018, Washington joined ZERO TO THREE’s IECMH Financing Policy Project (IECMH-FPP). The goal of the IECMH-FPP was to advance state financing policy related to IECMH through the provision of technical assistance and facilitation of a national learning collaborative. The Washington IECMH-FPP team was comprised of representatives from the HCA, Department of Health, Department of Early Learning (now the Department of Children, Youth, and Families), clinicians, and the executive director of the Washington Association for Infant Mental Health.
As part of the IECMH-FPP, state teams were required to develop a workplan detailing their goals for this work. Washington identified that the highest priority was legislation requiring that DC:0–5 be used for assessment and diagnosis of children birth to 5. Washington reviewed other states’ models for funding DC:0–5 trainings and explored the policy changes necessary to make DC:0–5 the required assessment and diagnostic tool for birth to 5 providers in the state. The state team also investigated ways to increase the number of reimbursable assessment sessions. During this time, CYBHWG formed a Prenatal to Five Relational Health Subcommittee in which many members of the IECMH-FPP team participated. Recommendations from the IECMH-FPP team were brought to the subcommittee, which were in turn brought to the CYBHWG.
Following recommendations from the CYBHWG, the legislature appropriated funds in the 2020 budget for the HCA to complete a cost analysis of implementing DC:0–5 statewide. For the 2021 legislative session, the CYBHWG produced a report with recommendations to the legislature (developed by approximately 200 individuals), which included statewide implementation of DC:0–5; the cost analysis was instrumental in informing the fiscal estimates associated with this recommendation and the resulting legislation. In April 2021, HB1325: Implementing Policies Related to Children and Youth Behavioral Health was signed into law.
These efforts would not have been possible without the support of key champions including CYBHWG, University of Washington (Partners for Our Children), Medicaid staff, Perigee Fund, Washington Association of Infant Mental Health, Washington legislators, and IECMH clinical providers.
Strategic Tips
- Build relationships. Talk to other states about strategies that have worked, and challenges experienced. Find a specific person who is willing to answer questions and collaborate. Connections with other states are so important.
- Trust the process. Be confident that the work is making a difference. It may feel like the process is taking a long time, but every small step matters.
- Engage IECMH champions. It is important to engage fiscal staff and IECMH champions who not only understand the intent of the policy but also the needs of providers and families. Their expertise is invaluable.
- Learn about and listen to opposing groups. Understanding the opposing perspectives can help strengthen the argument for changes and prepare for last-minute opposition.
Key Challenges
- Aligning practice with legislation. This will entail training providers in DC:0–5 and developing a crosswalk, as ICD-10 codes will still be required for billing purposes.
- Limited training capacity. There are currently two DC:0–5 trainers in Washington, which will impact the number of providers that can be trained and the timeline.
- Need for sustainability plan. Legislation funds will conclude after 2 years, which will require the development of a long-term plan to continue the work.
- Scope of Funds. The legislation limits funding to therapists to receive the Clinical DC:0–5 training. Separate funding is available for allied professionals (e.g., IECMH consultants) to receive the DC:0–5 Overview Training.
- Limited IECMH workforce capacity. Due to the shortage of IECMH professionals, providers who work primarily with older children or adults may need to be trained in DC:0–5; however, they may not have had opportunity to gain foundational knowledge around IECMH.
Lessons Learned
- Produce a cost analysis of DC:0–5 to inform state legislation. Involve staff who understand the intent of the policy and the needs of providers and families.
- Include ancillary pieces in the budget such as funding for trainings on IECMH foundations and/or observation tools, logistics of trainings (e.g., ZOOM and marketing), and evaluation.
- Carve out a space for the prenatal to 5 population and ensure their needs are strongly represented in groups working on broader children’s issues. It is important to advocate for more funds for all groups.
- Explore a variety of strategies by consulting with other states. Other states have been successful in integrating DC:0–5 into their state policy and systems, each using a different strategy. If it is necessary to prioritize (e.g., billing vs. training aspect), think about the best ways to distribute available fiscal and personnel resources.
- Explore different opportunities to optimize financing for training, such as through legislatively allocated state funds, Community-Based Mental Health Block Grant funds, or other grant programs. If training is targeting Medicaid providers, work with Medicaid financial experts to discuss whether training activities are allowable for federal match (e.g., Federal Financial Participation).
- Collaborate and consult with subject matter experts on the Medicaid State Plan. Medicaid’s implementation has variability across states. Becoming familiar with the Medicaid State Plan can provide insights around where and how mental health services are being implemented within the state’s system.

The social–emotional health of infants and young children is closely intertwined with that of their parents and other caregivers. Photo: shutterstock/violetblue
For More Information
Christine Cole, IECMH Program Manager, Washington State Health Care Authority, christine.cole@hca.wa.gov
Kiki Fabian, IECMH Systems Analyst, Washington State Health Care Authority, kiki.fabian@hca.wa.gov
HB2439: Increasing Access to Adequate and Appropriate Mental Health Services for Children and Youth
HB1325: Implementing Policies Related to Children and Youth Behavioral Health
Cost Analysis: Behavioral Health Assessment and Diagnosis for Infants and Children
Children and Youth Behavioral Health Work Group Recommendations (2016–2020)
State Policy Story: Nevada
EHRs are preloaded with DSM-5 and ICD-10 diagnostic codes. When treating infants and young children, a crosswalk is often used to allow billing and reimbursement. The EHR displays either the DSM-5 or the ICD-10 code. However, use of these codes does not provide accurate diagnostic information or allow tracking of treatment for specific diagnoses of infants and young children. Nevada is one of the first states to embed DC:0-5 into their EHR system, and the first state to embed DC:0–5 into MyAvatarTM.
The Innovation
Following the publication of DC:0–5, Nevada hoped to update their EHR system, MyAvatar, to include DC:0–5 diagnoses. MyAvatar now has a look-up field where clinicians can search for the term associated with each DC:0–5 Axis 1 diagnosis that is cross-mapped to the ICD-10 code for billing purposes.
The Impetus
Nevada began their IECMH work several decades ago. Advocates were successful in including Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood: Revised Edition (DC:0–3R; ZERO TO THREE, 2005) language into the state’s Medicaid manual in 2005. This language has since been removed; however, advocates are hopeful it will be reinstated. By 2007, Nevada Health & Human Services Division of Child & Family Services (DCFS) had embedded DC:0–3R diagnoses into MyAvatar. (See Box 2).
To ensure providers were familiar with DC:0–3R, approved trainers conducted multiple trainings per year. With the release of DC:0–5 in 2016 staff needed to be re-trained, so an internal training was developed. In 2017, DCFS began working to update MyAvatar with the new DC:0–5 diagnoses following a DC:0–5 training.
The Process
DCFS reached out to Netsmart with the hope of adding custom DC:0–5 diagnoses into MyAvatar. Because there is a universal dictionary shared across all the Intelligent Medical Objects (IMO) clients as well as 500 Netsmart clients, it is not as easy as just updating the system. Clinicians from Nevada, staff from Netsmart, and the clinical staff from IMO were involved in the discussions that began in 2018. DCFS sent Netsmart a spreadsheet with the majority of DC:0–5 diagnoses and the ICD-10 mapping. Netsmart reviewed the content to determine whether the presented content was included in IMO’s list and matched their existing DSM-5 to ICD-10 crosswalk, and sought guidance from their clinical team when terms were missing or did not match. For most missing terms, it was an easy conversation to ensure that the DC:0–5 diagnosis matched their coding guidelines, and the clinical staff were comfortable with the ICD-10 code that it matched to. A few terms took more time but, for the most part, the key players were able to reach agreement.
Netsmart now has a look-up field where clinicians can search for terms associated with the DC:0–5 Axis 1 diagnosis. After a term is searched, it will populate the agreed-upon search term (which is a term from the Axis 1 diagnosis) to cross-map to ICD-10. The cross-mapped ICD-10 diagnosis is used for billing purposes and is maintained in the EHR. DCFS developed specific internal reports, documenting the treatment plan and psychosocial assessment, that are cross-mapped to the DC:0–5 search term. This cross-mapping allows for the DC:0–5 search term to populate the report instead of the ICD-10 diagnosis. Narrative fields were added to the reports to allow for the DC:0–5 diagnosis to be captured there.
Box 2. Key Terms
Netsmart provides electronic health record technology, health care software solutions, and professional services for human services and post-acute communities.
MyAvatar is an electronic health record specifically designed for organizations that provide behavioral health and addictions treatment services in community-based, residential, and inpatient programs.
Intelligent Medical Objects is a company specializing in developing, managing, and licensing medical vocabularies.
Providers had to be trained to use DC:0–5. A Health Resources & Services Administration grant for pediatric access funded the official DC:0–5 training for providers and the community. Internal DCFS staff and external providers were invited to various trainings across the regions from October 2019 through September 2021. Approximately 125 individuals have been trained including marriage and family therapists, licensed social workers, psychologists, interns, university staff, early intervention staff, and child welfare staff. A System of Care grant (targeting rural and frontier populations) funded another DC:0–5 Train the Trainer in the fall of 2021.
Nevada is investigating how to capture developmentally appropriate data now that DC:0–5 is embedded in MyAvatar. Users have been able to access the final diagnosis at discharge but did not have a way to access the admission or post-foundational diagnosis. Nevada is currently working on implementation of an additional section within MyAvatar called “post-foundational diagnosis” which will allow providers to input the DC:0–5 diagnosis given after three to five contacts with the family. Capturing this data will be a significant contribution in advancing IECMH policy and systems.
Due to Nevada’s efforts, any organization across the country using MyAvatar may now access the Nevada cross-map to ICD-10 by using the DC:0–5 search terms. These efforts would not have been possible without the support of key champions including DCFS staff and representatives from Netsmart and MyAvatar.
Strategic Tips
- Be patient. Persistence and perseverance are key. Do not assume people know about IECMH. Educate the community.
- Include DC:0–5 in the Medicaid State plan, to allow users to become familiar with DC:0–5 and its value.
- Embed DC:0–5 into various grants to increase DC:0–5 exposure beyond an individual agency. Think about the bigger picture and covey ideas on paper.
- Build capacity by training internal staff as trainers.
Key Challenges
- Copyright concerns. Netsmart expressed copyright concerns regarding DC:0–5 and opted to input key search terms rather than the full DC:0-5 diagnoses.
- Lack of understanding. There was push back around the need to include DC:0–5 diagnoses in the EHR because of the pre-existing cross-map from DSM-5 to ICD-10. Netsmart had never received this type of request from any other state. Stakeholders had to demonstrate that DC:0–5 was the recognized diagnostic classification for infants and young children.
- Barriers to training pediatricians. The time commitment and lack of incentive prevent pediatricians from attending DC:0–5 trainings. Continuing Medical Education credits are expensive to offer.
- Lack of IECMH expertise. Many of the providers trained in DC:0–5 did not have a background in IECMH.
Lessons Learned
- Capitalize on the work of other states and ask for help when needed. The IECMH-FPP Basecamp platform has been an incredible resource. Connecting with other states and having access to shared tools and information have helped advance efforts.
- Identify champions and continue to feed them information. It is important to build those relationships over time.
- Have a vision and brainstorm ideas before opportunities arise. It takes time to determine what the community wants and needs.
- Pursue every opportunity that comes your way. Be open to exploring new opportunities to advance the work. Opportunities present themselves every day.
For More Information
Krisann Alvarez, PhD, Licensed Psychologist, Nevada Health & Human Services Division of Child & Family Services, kAlvarez@ dcfs.nv.gov
Rhonda Lawrence, LMFT, Clinical Program Manager II, Nevada Health & Human Services Division of Child & Family Services, rlawrence@dcfs.nv.gov
Ann Polakowski, LCSW, Clinical Program Manager II, Nevada Health & Human Services Division of Child & Family Services, apolakowski@dcfs.nv.gov
State Policy Story: Massachusetts
All states are concerned with shortages of qualified child psychiatrists, psychologists, and other mental health providers. To build workforce capacity, promote widespread use of DC:0–5, and improve professional knowledge about IECMH disorders, states can include DC:0–5 in a broader early childhood workforce development strategy. Providing training on DC:0–5 and IECMH treatment strategies can help to ensure access to a cadre of qualified mental health clinicians. DC:0–5 training can also be helpful for professionals who do not diagnose, so they are able to recognize signs that a child needs additional supports or assessment. Massachusetts braided funds and engaged a multidisciplinary group of clinicians, policymakers, and influencers to advance DC:0–5 professional development efforts across the state.
The Innovation
Massachusetts is working to advance DC:0–5 professional development efforts across the state by engaging a multidisciplinary group of clinicians, policymakers, and influencers; creating public–private partnerships; and braiding funds (see Box 3). With the support of several state agencies and private organizations, Massachusetts has developed a streamlined system for the delivery of professional development and implementation support, founded in workforce diversity, equity, and inclusion.
The Impetus
Over the past decade, policymakers and stakeholders in Massachusetts advanced an IECMH agenda. In 2016, Massachusetts joined the ZERO TO THREE IECMH-FPP, with the goal of building a public–private partnership to coordinate efforts across the two sectors and to move the policy work forward. The team worked to build buy-in from other stakeholders and to develop three to five policy levers, with widespread education about and uptake of the DC:0–5 becoming one of the most important. During a policy forum held by the state team in 2017, attendee stakeholders proposed a pilot training for providers working across settings, including outpatient mental health, early intervention, and other community-based behavioral health settings.
The Process
Massachusetts’ DC:0–5 professional development efforts began in 2017. A Project LAUNCH (Linking Actions for Unmet Needs in Children’s Health) grant through the Department of Public Health (DPH) provided funding for a DC:0–5 training for LAUNCH clinicians and family partners; several slots were offered to policymakers and influencers. Including policymakers and influencers at this first training proved to be politically strategic in advancing DC:0–5 professional development efforts across the state. Two lessons learned from this training were that further follow-up was needed to support implementation of DC:0–5 and that there were questions around billing which needed to be addressed.
Box 3. The Massachusetts IECMH-FPP Team
The Massachusetts Infant and Early Childhood Mental Health Financing Policy Project team includes:
• MassHealth—Massachusetts’ combined Medicaid and CHIP program
• Department of Early Education and Care
• Department of Mental Health (DMH)
• Department of Public Health (DPH)
• Children’s Mental Health Campaign —A statewide policy and advocacy network
• A child psychiatrist
A pilot was developed that included DC:0–5 training and follow-up consultation in the form of onsite technical assistance and reflective case consultation webinars. The pilot workgroup included DPH (lead), MassHealth’s Office of Behavioral Health, Departments of Mental Health and Early Education and Care, and the Children’s Mental Health Campaign. State policy leaders braided funding to make this possible: the Department of Mental Health (DMH) paid for the training, while DPH’s Project LAUNCH paid for books and consultation and coordinated the effort. Feedback was gathered from attendees throughout the pilot that informed subsequent trainings. For example, attendees reported that reflective case consultation is effective for teams to put DC:0–5 into practice and is now a permanent component of the trainings due to the overwhelmingly positive feedback.

Adopting an age-appropriate diagnosis and treatment classification system is an important step toward assuring better overall health for infants, young children, and their families. Photo: shutterstock/Ann Rodchua
The success of the pilot resulted in support from MassHealth that included funding for several new trainings and a grant to support case consultation. Over the past 5 years, DPH, the Boston Public Health Commission, and MassHealth sponsored six large DC:0–5 trainings; 360 professionals (mental health clinicians, family partners, psychiatrists, pediatricians, policymakers, and influencers) participated—more than 100 of whom also participated in DC:0–5 reflective case consultation webinars.
To achieve more widespread access to DC:0–5 training, MassHealth used a “train the trainer” model, requiring that participants commit to providing at minimum one free training in their community following certification. Since then, seven new trainings led by the trained in-state trainers have been supported by MassHealth.
There are currently two full-time staff (DMH and Massachusetts Association for Infant Mental Health/Massachusetts Society for the Prevention of Cruelty to Children) dedicated to supporting IECMH work in the state, providing increased capacity for policy and program development. The staff represent the public–private partnership that has brought the work this far, and they work together to coordinate DC:0–5 trainings and diversity, equity, and inclusion-centered outreach efforts. They also created an online hub to connect trainers across the state, to share resources, and to facilitate coordination of requested trainings and reflective case consultation.
These efforts would not have been possible without the support of key champions including the IECMH Interagency Policy Workgroup (particularly the DC:0–5 subcommittee and the DC:0–5 Professional Development subcommittee), MassHealth, the Executive Office of Health and Human Services, Boston Public Health Commission, the Massachusetts Association for Infant Mental Health, the Massachusetts Society for the Prevention of Cruelty to Children, and the Massachusetts IECMH-FPP state team (including representatives from MassHealth, Department of Early Education and Care, DMH, DPH, and the Children’s Mental Health Campaign).
Strategic Tips
- Pursue relentless incrementalism. Focused and consistent marginal improvements over time make a big cumulative impact. Be patient. Policy and systems change take time.
- Determine the key influencers. Find the key influencers who can help move the needle. Communicate and coordinate efforts to be the most strategic about moving the work forward. Tap into the expertise and support of advocacy partners and policymakers.
- Build private–public partnerships. Lean into relationships to deepen partnerships. Be intentional and centered on relationships and bring a chair to tables that IECMH has been missing from.
- Braid funding. Look at ways to use in-kind resources. Having multiple agencies involved in the effort produces a greater level of buy-in.
Key Challenges
- Billing. Some clinicians report that the fee-for-service billing system does not always adequately compensate providers for the time spent performing documentation, particularly for providers conducting additional assessments, such as DC:0–5, which takes three to five sessions to perform.
- “The knot”. It is not easy to balance and consider the perspectives of multiple parties, including billing staff, managed care companies, clinicians, and Medicaid. There are different levels of understanding of the dyadic nature of IEMCH assessment and diagnosis, treatment, and billing. The knot represents an issue that can’t be resolved because it has gotten so entangled and taut that the different threads can’t be untangled. IECMH practitioners experience challenges in billing for their work, partly due to multiple parties (including billing staff, managed care companies, clinicians, and insurers) bringing differing points of view about the nature of services and how they are billed.
- Lack of infrastructure. There has been a dearth of stable funding, clear pathways, and expectations around IECMH services and supports. Recent policy developments, such as the state’s Behavioral Health Roadmap and MassHealth policy allowing for payment for preventative behavioral health services, may help to address this concern.
Lessons Learned
- Include reflective case consultation as part of the training package. The team has received consistent positive feedback about this component.
- Be intentional about diversity, equity, and inclusion as the foundation for implementation and coordination efforts. This work should diversify and strengthen the workforce.
- Increase accessibility with virtual training for providers as travel and lodging costs are not always feasible. The plan is to keep a virtual training option moving forward.
- Think about relationships in every sense when it comes to policy, implementation, and reaching providers. There have been no issues filling the trainings and reaching providers. It is critical to know who to ask and where to publicize.
- Focus on outreach and be intentional with communication and marketing efforts. The development of a statewide IECMH newsletter has helped with reaching new partners.
- Connect with other states and share ideas. ZERO TO THREE DC:0–5 Community of Practice monthly calls have been helpful for individual trainers and collectively as a state to learn from other states.
For More Information
Andrea Goncalves Oliveira, Infant and Early Childhood Mental Health Statewide Coordinator, Massachusetts Department of Mental Health, andrea.goncalves-oliveira@mass.gov
Kate Roper, Director of Early Childhood Services, Massachusetts Department of Public Health, kate.roper@mass.gov
Aditi Subramaniam, Associate Director, Infant Early Childhood Mental Health, Massachusetts Society for the Prevention of Cruelty to Children, asubramaniam@mspcc.org
Margot Tracy, Youth and Family Manager, MassHealth, margot. tracy@mass.gov
The Partnership for Early Childhood Mental Health: http://www.ecmhmatters.org/Pages/ECMHMatters.aspx
Conclusion
This article provides a point-in-time perspective on how some states are integrating DC:0–5 into state policy and systems. These state policy stories demonstrate the innovative work taking place across the country 5 years following the publication of DC:0–5. Many other states are working to integrate DC:0–5 into IECMH policy and practice and to improve the availability and quality of IECMH services and supports. Adopting an age-appropriate diagnosis and treatment classification system is an important step toward assuring better overall health for infants, young children, and their families.
Author Bios
Julie Cohen, MSW, is associate director of the ZERO TO THREE Policy Center. During her more than two-decade career at ZERO TO THREE, Ms. Cohen has worked on a wide range of policy issues impacting infants and toddlers, including infant and early childhood mental health (IECMH). She is currently a member of the IECMH Policy Team. She was a member of the international expert workgroup that wrote DC:0–5TM:Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood . Her portfolio at ZERO TO THREE includes: implementing strategic initiatives and conceptualizing new IECMH projects; overseeing and developing policy briefs, research briefs, articles, guides, memos, blogs, and other resources on IECMH policy; and assisting policymakers and their staff as a technical resource. She is the author of numerous publications.
Paola Andujar, MS, is a policy analyst with the ZERO TO THREE Infant and Early Childhood Mental Health (IECMH) Policy Team. Ms. Andujar has more than 6 years of experience in the field of early childhood and maternal health. She has supported IECMH systems-building efforts at the state and national levels and the work of Tribal home visiting grantees across the country. Her experiences include training and professional development within home visiting; coordination of technical assistance; research; and resource development, including policy briefs, newsletters, and other publications. She is skilled in grant management, programmatic support, stakeholder engagement, and communication platforms.
Suggested Citation
Cohen, J., & Andujar, P. (2021). Integrating DC:0–5 into state policy and systems: 5 years of progress. ZERO TO THREE Journal, 42(2), 40–48.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental health disorders (5th ed.).
World Health Organization. (1992). International classification of diseases (10th ed.).
ZERO TO THREE. (2005). Diagnostic classification of mental health and developmental disorders of infancy and early childhood (rev. ed.).
ZERO TO THREE. (2016). DC:0–5TM: Diagnostic classification of mental health and developmental disorders of infancy and early childhood (DC:0–5).