Tanika Eaves, Fairfield University
Abstract
This article is a call to action to the infant mental profession to consider infant mental health (IMH) practice as care work that is often marginalized in contemporary American society. The author examines critical elements of care work that juxtapose competent IMH practice. Investigating the experiences of those performing IMH work is necessary to better understand what support and resources the IMH workforce needs to grow and thrive, and what the best mechanisms might be for addressing imbalances in power and privilege between IMH practitioners and the families they serve.
The infant mental health (IMH) profession is grounded in relationship-based work with infants, young children, and families within a socioecological framework (Walsh et al., in press). For the purposes of this article, the IMH field refers to the wide range of professionals who support and care for children and their families, including early education settings (child care, preschool, early intervention); home visiting, child welfare, and other family support programs; health care providers; and clinical mental health services, such as social workers and therapists.
Inequities in IMH Practice
In all of these roles and settings, caring is at the essence of IMH practice. The inequities existing in who practices direct IMH work on the frontline and who typically receives IMH services are defining elements of care work. In other words, women dominate frontline IMH practice. They often perform care for marginalized families for low pay despite being highly skilled and trained. This reality highlights the marginalization of the IMH field and is one illustration of how care work is gendered, de-skilled, and devalued in contemporary American culture (Charlesworth et al., 2005; Duffy, 2007; England, 2005). The current sociopolitical climate amid a global pandemic calls for a critical examination of IMH practice as care work through a social justice lens.
A Divided Nation
The 2020 election cycle has been marked by a year of sharp political divisions, economic downturn, and awakening to systemic racism most starkly demonstrated by numerous cases of police brutality and killings of black and brown American citizens. These elements, exacerbated by a global public health crisis, have only served to push the most vulnerable young children and families further into the margins. In fact, the COVID-19 pandemic has exposed and illuminated existing inequities along the lines of class, gender, and race.
The typically lower-wage earning essential workforce has been on the frontlines during the pandemic and is also more likely to suffer from job and income loss. As of October 2020, 865,000 women, mostly mothers ( http://Nextgov.com, 2020) have had to leave the workforce to care for and homeschool children, and it is unclear if the jobs they left will still exist when they return. Finally, issues like health care access, education, housing, and income wealth gaps place people from racial minority groups at a disproportionately increased risk of hospitalization and death from COVID-19 (Centers for Disease Control and Prevention, 2020).
The Impact of COVID-19 on IMH Practice
Although the impact of COVID-19 on infant–family systems service delivery is still evolving, anecdotal accounts suggest that the move from largely in-person contact to telehealth is not without complications. Concerns about enrollment, engagement, and retention of families that may already be hard to reach in a virtual realm have arisen (Traube et al., 2020). In addition, practitioners worry that telehealth may impede relationship building and obscure potential crises in the highneed families that they serve.
For both families and practitioners, the pandemic has further exacerbated inequities as vulnerable families receiving IMH services may be more likely to rely on early childhood education and other infant–family program providers, placing both groups at increased risk for contracting COVID-19. Furthermore, as programs shift to a telehealth model of service delivery, disparities in access to care in terms of whether or not families have stable Internet connection, reliable devices, and availability for online sessions raise more questions and concerns about inequities in privilege and accessibility of services and support during a critical time.
Defining Care Work
To better understand the unique position of frontline IMH service delivery as care work, Bubeck (1995) offered a multifaceted definition of care. This definition drew from earlier theoretical frameworks (Graham, 1983; Noddings, 2003) to examine four key aspects of care:
- care as an activity: the attention to the physical and emotional needs of another;
- the psychology of care: the psychological and emotional rewards and costs associated with caring work;
- the ethic of care: caring as an attitude characterized by emotional investment rather than as an activity (Noddings, 2003); and
- the gendered nature of care: care as “women’s work” (Bubeck, 1995, p.60).
The benchmarks of effective practice and IMH competency (i.e., relationship-based, culturally competent, multidisciplinary infant and early childhood mental health service delivery which emphasizes working with others, communicating, thinking, and reflecting; Weatherston et al., 2009) encompass the first three key aspects of care. The earliest roots of IMH practice began in the homes of parents and infants in need of relational care. This form of kitchen table therapy, coined by IMH pioneer Selma Fraiberg (Fraiberg et al., 1975) capitalized on the practitioner’s caring for the mother–infant dyad and required laser-focused attention to their physical and emotional needs.
IMH practice, because of its intimate, relational nature, is rife with psychological and emotional costs and rewards. Every IMH practitioner experiences the ups and downs of working with vulnerable children and families and feels varying degrees of stress and secondary trauma (the impact of indirect exposure to difficult, disturbing, and/or traumatic images and stories of the suffering of others) coupled with satisfaction derived from performing their work. Furthermore, IMH competency and effective practice is impossible without the ethic of care. That is, IMH practitioners are not just performing intervention as an activity, rather they are invested in secure, healthy beginnings for the infants, young children, and families they care for. The fourth key aspect of caring, the gendered nature of care as “women’s work” (Bubeck, 1995) is also inherent in IMH practice given the over-representation of women holding frontline IMH practitioner positions (St. John et al., 2012).
Care in a Patriarchal, Capitalist Society
Bubeck (1995), purported that much of “women’s work is not understood as production or profitable, but rather as care; an activity aimed at meeting the needs of others” (p. 9). Cultural norms in a patriarchal, capitalist society may perceive female-dominated careers as less skilled and less professional, hence devaluing (and undercompensating) the care work IMH practitioners perform and that is essential to a thriving society.
More than just possessing skills essential to competent IMH practice, the IMH practitioner must be adept at developing and maintaining relationships (Weatherston et al., 2009). In other theories of care in feminist scholarship, it is relationship development and maintenance that is fundamental to the performance of care (England, 2005, Hochschild, 2003; Tronto, 2010). Furthermore, within a capitalist framework emphasizing production and materialism, relationship-based care work becomes exploitable. Feminist scholars theorize that this is because care is typically believed to embody feminine characteristics in Western culture (Duffy, 2007; England, 2005). Hence, care work is largely rendered as “women’s work” (Bubeck, 1995, p.60). Cultural assumptions postulate that caring comes more naturally to women than men, that women are nurturers by nature and therefore, care work can be perceived less as work, and more as vocation or a calling where economic compensation, productivity, and the benefit of care work to the larger society are minimally considered (Bubeck, 1995; Duffy, 2007; England, 2005). Further, those performing care work, and those in need of care work, are often members of society’s most vulnerable and marginalized populations (Duffy, 2007; England, 2005; Hochschild, 2003; Wharton, 2009).
Finally, the devaluation of care work in general, and the feminization of care labor in particular, come together in the care theories work of Charlesworth et al. (2015) and Duffy (2007), which argued that female human service professionals (those performing care work in particular), are the most stressed and strained members of the workforce because they are often juggling intense care needs in their relatively low-paying jobs and in their personal lives, with very little support from institutions to strike a healthy balance.

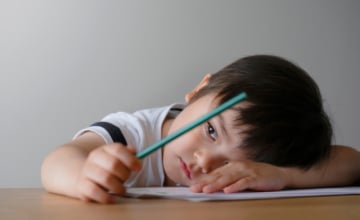
Practitioners worry that telehealth may impede relationship building and obscure potential crises in the high-need families that they serve. Photo: shutterstock/Dragon Images
Who Performs Care Work in the IMH Field?
What do leaders in the IMH field know about the performance of care and the delineation of levels at which IMH practitioners perform care along lines of class, education, and race? It is widely assumed that women are over-represented in the IMH field at the frontline practitioner level (St. John et al., 2012). However, what do researchers know about who these women are and the life experience they bring to the work? Do women of color tend to occupy positions requiring less education and training and perform more physical care tasks in early childhood education, family child care homes, or home visiting settings? Can it be assumed that White, middle- and upper-middle-class women are over-represented in clinical and specialist frontline IMH positions, and tend to be more likely to hold supervisory and administrative roles? St. John and colleagues’ 2012 article “Infant Mental Health Professional Development: Together in the Struggle for Social Justice” explored how these assumed demographic trends are associated with a high prevalence of “cultural mismatching” between practitioners and vulnerable infants, young children, and families where the frontline practitioner is typically from the dominant cultural group in American society and the family served is from a marginalized group. However, there are little data that describe what the IMH frontline workforce looks like demographically. Furthermore, this lack of information is a hindrance to adequately answering questions about what sorts of supports and resources the IMH workforce needs to grow and thrive, and what the best mechanisms might be for addressing imbalances in power and privilege between IMH practitioners and the families they serve.
Implications
The apparent gender disparity within a care-oriented workforce charged with promoting optimal psychosocial outcomes for the youngest, most vulnerable, and often marginalized children and families, coupled with the inherent invisibility of the IMH profession within contemporary American society (Lally, 2013), raises questions about IMH professionals’ responsibility as advocates and leaders in the field. How do they give voice to the position of IMH as an interdisciplinary field of innovative practice, scientific inquiry, and progressive policy development key to mobilizing society toward equity and social justice? Perhaps the time has come for program planners and administrators of infant- and family-serving systems to take pause and notice whether or not frontline and leadership staff are representative of the families and communities targeted for service. Perhaps researchers might ask themselves if they unintentionally privilege narrow, antiquated norms and definitions of family composition, family functioning, and parenting when they recruit participants and design assessment tools and interventions meant to strengthen families.
At this particular point in America’s social history, those who are committed to a just, equitable, healthy society for all babies and families must turn a critical eye inward and examine in what ways actors in the IMH profession may be reproducing inequities and marginalization within the workforce. The first step might be systematically investigating who is performing IMH work, who identifies as an IMH professional, and what their experiences have been working in the field given their particular social location and perspective. At this seminal moment in culture and society, the IMH community has an opportunity to reflect on parallel processes of marginalization and invisibility of babies and families in contemporary American society, and the devalued position of IMH practice within the broader professional hierarchy of the job market. Americans must ask themselves
- “What are the priorities of our nation?”
- “Who sets the priorities and how is the IMH field aligned, or not aligned?”
- “Who decides what kind of work is valuable?”
- “How do we determine who is deserving of respect, recognition, and comparable pay for the work they perform?”
and finally, they must all grapple with the question of what kind of society they want our children to grow and develop in.
A society that fails to invest in its children, families, and the workforce who cares for them, is a society with a grim future.
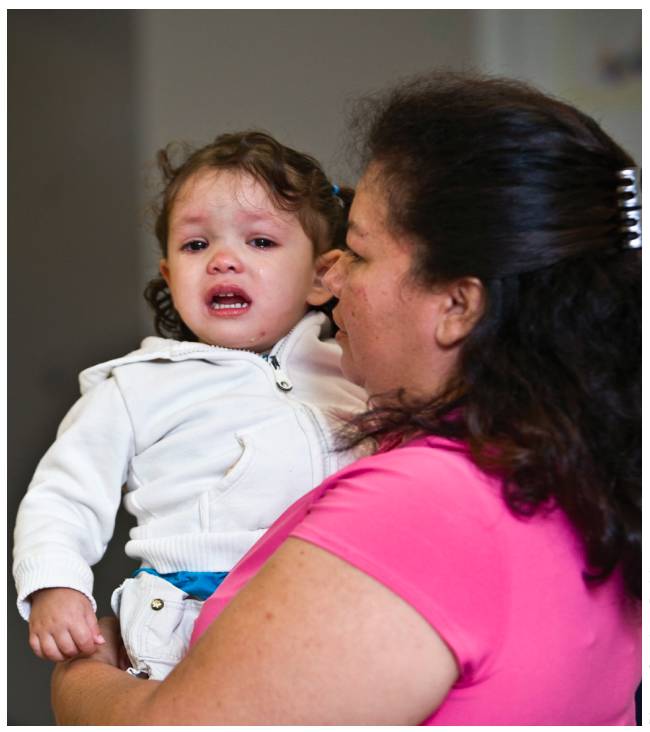
Infant mental health practitioners are not just performing intervention as an activity, rather they are invested in secure, healthy beginnings for the infants, young children, and families they care for. Photo: Stephen Bobb
Learn More
The Diversity-Informed Tenets for Work with Infants, Children and Families
https://diversityinformedtenets.org/the-tenets/overview
Social Justice Resources—Children’s Community School
www.childrenscommunityschool.org/social-justice-resources
Center on the Developing Child-Harvard University: A Guide to COVID-19 and Early Childhood Development
https://developingchild.harvard.edu/resources/how-to-support-children-and-yourself-during-the-covid-19-outbreak
Child Mind Institute—Telehealth for Kids
https://childmind.org/article/telehealth-for-kids
Our Economy: What Is “Care Work?”
www.ecnmy.org/learn/your-livelihood/paid-vs-unpaid/what-is-care-work
Suggested Citation
Eaves, T., (2020). Perspectives: Who cares? The parallel process of marginalizing babies, families, and infant mental health practice as care work. ZERO TO THREE Journal, 41(2), 54–58.
Author
Tanika Eaves, PhD, LCSW, IMH-E®, is an assistant professor of social work at Fairfield University Egan School of Nursing and Health Studies. Dr. Eaves has a bachelor of arts in psychology from Fairfield University, a master’s of social work from Rutgers University, and a doctor of philosophy in human development and family science from the University of Connecticut. Dr. Eaves has been a licensed clinical social worker for more than 20 years, and holds the Connecticut Association for Infant Mental Health Endorsement as an Infant Mental Health Specialist. Her professional experience includes: direct clinical services in child and family guidance clinics, early intervention programs, early childhood mental health consultation, parent– infant psychotherapy, policy development, and training/ consultation with home visiting clinicians. Dr. Eaves’ research investigates individual and organizational factors impacting work-related stress management among frontline and supervising infant mental health practitioners.
References
Bubeck, D. E. (1995). Care, gender, and justice. Clarendon Press. Centers for Disease Control and Prevention. (2020). Coronavirus disease 2019. www.cdc.gov/coronavirus/2019-ncov
Charlesworth, S., Baines, D., & Cunningham, I. (2015). ‘’If I had a family, there is no way that I could afford to work here”: Juggling paid and unpaid care work in social services. Gender, Work and Organization, 22(6), 596–613.
Duffy, M. (2007). Doing the dirty work: Gender, race, and reproductive labor in historical perspective. Gender & Society, 21(3), 313–336. http://doi.org/10.1177/0891243207300764
England, P. (2005). Emerging theories of care work. Annual Review of Sociology, 31, 381–399, http://doi.org/10.1146/annurev.soc.31.041304.122317
Fraiberg, S., Adelson, E., & Shapiro, V. (1975). Ghosts in the nursery: A psychoanalytic approach to problems of impaired infant-mother relationships. Journal of the American Academy of Child Psychiatry, 14, 387–421.
Graham, H. (1983). Caring: A labor of love. Finch & Groves.
Hochschild, A. R. (2003). The managed heart: Commercialization of human feeling. University of California Press.
Lally, R. (2013). For our babies: Ending the invisible neglect of America’s infants. Teacher’s College Press.
Nextgov.com (2020). 865,000 women left the workforce last month. www.nextgov.com/cio-briefing/2020/10/865000-women-left-workforce-last-month/169015
Noddings, N. (2003). Caring: A feminine approach to ethics and moral education (2nd ed.).University of California Press. (Original work published 1984)
St. John, M. S., Thomas, K., & Norona, C. (2012). Infant mental health professional development: Together in the struggle for social justice. ZERO TO THREE Journal, 33(2), 13–22.
Traube, D. E., Hsiao, H., Rau, A., O’Brien, D. H., Lu, L., & Islam, N. (2020). Advancing home based parenting programs through the use of telehealth technology. Journal of Child & Family Studies, 29, 44–53. https://link.springer.com/article/10.1007/s10826-019-01458-w
Tronto, J. C. (2010). Creating caring institutions: Politics, plurality, and purpose. Ethics and Social Welfare, 4(2), 158–171. https://doi.org/10.1080/17496535.2010.484259
Walsh, T., Paris, R., Ribaudo, J., & Gilkerson, L. (in press). Locating infant and early childhood mental health at the heart of social work. Social Work.
Weatherston, D., Kaplan-Estrin, M., & Goldberg, S. (2009). Strengthening and recognizing knowledge, skills, and reflective practice: The Michigan Association for Infant Mental Health competency guidelines endorsement process. Infant Mental Health Journal, 30(6), 648–663.
Wharton, A. S. (2009). The sociology of emotional labor. Annual Review of Sociology, 35, 147–165.