Yael Dai, University of Massachusetts Boston
Daina M. Tagavi, University of Washington
Alice S. Carter, University of Massachusetts Boston
Abstract
Early diagnosis of autism spectrum disorder (ASD) facilitates access to interventions that improve outcomes for children and families. Understanding developmental and behavioral manifestations of symptoms and competencies improves early diagnosis. The authors illustrate the benefits of using the ZERO TO THREE DC:0–5TM: Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood (DC:0–5, 2016) multiaxial system for assessment of young children suspected of having a diagnosis of ASD. DC:0–5 provides a framework for forming rich conceptualizations that reflect the influence of the family system, physical health, psychosocial stressors, developmental competence and co-occurring mental health symptoms and disorders, to promote accurate early diagnosis and enhance treatment planning.
Children can be reliably diagnosed with autism spectrum disorder (ASD) by 14 months old (Pierce et al., 2019). Inaddition, autism symptoms, including delayed or limitedsocial behaviors and communication, are often present in the first year of life in children who are later diagnosed with ASD (Webb & Jones, 2009). Early diagnosis is important becauseit facilitates access to intervention. Participation in intensive early intervention is among the most important predictors of progress in communication and daily living skills in children with ASD (Anderson et al., 2014; MacDonald et al., 2014; Orinstein et al., 2015; Rogers & Vismara, 2008; Rogers et al., 2014).
A Multiaxial System
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; American Psychiatric Association, 2013) is the most common classification system to diagnose ASD in the United States. DC:0–5TM: Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood (DC:0–5; ZERO TO THREE, 2016) is fully concordant with the DSM-5 criteria for ASD. Its innovation lies in the emphasis on using a developmentally based approach to classifying mental health and developmental delays during childhood. DC:0–5 also emphasizes that young children are embedded within multiple systems that must be considered during evaluation, diagnosis, and treatment planning. Accordingly, DC:0–5 includes a multiaxial system to complement a clinical diagnosis.
Axis I: Clinical Disorders
Axis I includes clinical disorders and a description of the symptoms necessary to meet diagnostic criteria. Axis I is closely aligned with DSM-5 (American Psychiatric Association, 2013). However, it includes notes about the ways that symptoms may manifest in infants and young children, in order to support accurate diagnosis during the first 6 years of life (birth through 5).
Axis II: Relational Context
DC:0–5 posits that early relationships are critical to all children’s development. Accordingly, Axis II of DC:0–5 focuses on the child’s dyadic relational context, rather than focusing solely on the child. Axis II also highlights the ways in which caregivers coordinate caring for the child within the family system (e.g., arranging for pediatrician visits). The effects of caregiver behavior on child development have been extensively documented, including in families with a child with autism (Baker et al., 2011; Ingersoll & Gergans, 2007; Karst & Van Hecke, 2012; Mandell et al., 2011; Siller & Sigman, 2002). Specifically, tension across caregivers can contribute to challenges in young children’s adaptation, mood, and behavior regulation, and is considered an increased risk factor for children with autism (Mazzoni et al., 2018; McHale & Rasmussen, 1998). Importantly, there is a bidirectional relationship between family functioning and child adjustment (Karst & Van Hecke, 2012; Mazzoni et al., 2018; McHale & Rasmussen, 1998). An important component of assessment includes interviewing caregivers and observing interactions between the child and caregivers and among caregivers in the family system.
Axis III: Physical Health Conditions and Considerations
As physical, neurodevelopmental, and mental health are interrelated, Axis III provides a framework for considering the impact of a child’s physical health on clinical symptoms. Axis III directs attention to caregiver pregnancy and perinatal complications that can have a direct influence on a child’s development. It is particularly important to consider and evaluate the physical health of a child with ASD, in light of the higher rates of medical conditions that may negatively impact development in children with ASD (Bauman, 2010). For example, neurological, gastrointestinal, sleep, metabolic, and hormonal disorders are highly comorbid with ASD (Bauman, 2010; Muskens et al., 2017). Some children with ASD express pain or physical discomfort through aggression or self-injurious behaviors, instead of using verbal communication (Bauman, 2010). Therefore, providers who work with children with ASD should actively promote routine medical assessments.
Axis IV: Psychosocial Stressors
Axis IV provides a framework for gathering information about important stressors that may influence a child, including social, economic, housing, employment, legal, or familial challenges. It is particularly important to gather information about psychosocial stressors during an evaluation for ASD because autism confers risk for psychosocial stressors. For example, caregivers of children with ASD report higher levels of marital discord and financial burden than caregivers of children without a disorder (Hartley et al., 2017; Serrata, 2012). Social stressors and identities also have a direct impact on identification, diagnosis, and prognosis of ASD. For example, children from low-income households (Mandell et al., 2005) and Latinx and Black children are diagnosed with ASD later and experience more difficulty accessing services (Magaña et al., 2013; Mandell et al., 2002).
Axis V: Developmental Competence
Finally, Axis V provides a framework for integrating information about a child’s emotional, social, cognitive, language/social communication, and motor skills. When diagnosing ASD, it is particularly important to consider a child’s mental age and the social communication behaviors that would be expected by that age (Martínez-Pedraza & Carter, 2009). Doing so helps the clinician to understand a child’s social behavior in relation to developmental prerequisites and to highlight a child’s relative strengths and areas to target during intervention.
Keeping the DC:0–5 axes and cultural formulation (see Box 1) in mind (Sarche et al., 2019), and adding appropriate corresponding assessments to obtain a more holistic picture of the child, helps enhance case formulation and form an individualized treatment plan that engages the family in the intervention. This comprehensive assessment paradigm also aligns with calls from the autistic self- and family-advocate communities to make early autism assessment and intervention more compatible with the growing neurodiversity movement (Schuck et al., 2021 ). Advocates argue that case formulations and resulting intervention goals should be personalized and based on a nuanced, balanced understanding of both autistic and neurotypical development and behavior in a variety of contexts. In addition, caregivers, particularly those of very young children, play a necessary part in the assessment process and in shaping the program of behavioral intervention for their child. By examining the child in their broader relational, social, and cultural contexts as part of the assessment process, providers can empower caregivers to make these important decisions in a way that incorporates family values and culture while also focusing on the child’s individuality.
Box 1. What Is a Cultural Formulation?
A cultural formulation helps a provider to appreciate the many ways in which a child’s development and behavior are shaped by cultural practices and values. As part of a comprehensive cultural assessment, the assessor should identify the: (a) cultural identity (e.g., nationality, degree of acculturation, race, ethnicity, religion, gender) of the child, primary caregivers, and secondary caregivers; (b) cultural conceptualizations of the child’s behavior (e.g., the caregivers’ interpretation of child behavior, their experience of the behavior, and their feelings toward various types of treatment); (c ) cultural features of vulnerability and resilience (e.g., the child’s primary and secondary caregivers, the caregivers’ perceptions of social support and stressors); and (d) impact of cultural differences between the provider and the family, and the way that this may impact provider biases or the family’s degree of comfort seeking treatment and disclosing personal information (see Sarche et al., 2019 and ZERO TO THREE, 2016, for more information on conducting cultural assessments).
Clinical Example
The example of Lucas1 and his family that follows illustrates how using the DC:0–5 multiaxial approach during diagnostic evaluations provides a rich conceptualization of a child suspected of autism by focusing attention on the systems that influence child development and functioning.
Presenting Information
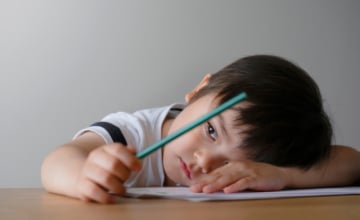
Lucas was a 14-month-old Latinx boy who was followed at an infant development follow-up clinic due to a history of premature birth and low birth weight. The clinic provides early, periodic interdisciplinary assessments and referrals for children from birth to 5 years old who are at high risk for neurodevelopmental and neurobehavioral problems. Lucas was previously evaluated using the Bayley Scales of Infant and Toddler Development Fourth Edition (Bayley-4; Bayley et al., 2019) at 6 months old. At that evaluation, Lucas’ cognitive, language, and motor scores on the Bayley-4 were within normal limits for his age. His mother, Mrs. Rivera, completed the present evaluation with Lucas. She reported that she had concerns about Lucas’ speech, difficulty falling asleep, and lack of engagement with her and his twin brother. Lucas’ mother noted she was proud of his ability to walk with support and his curiosity about objects. She reported that her husband, Mr. Rivera, was not interested in attending this evaluation. She explained that he is not concerned about Lucas’ development and believes that Lucas is just slow to progress and will “catch up eventually.”
1The clinical presentation of Lucas and his family is based on our composite experiences; We have combined features of many children and families to present a meaningful case example of the use of DC:0–5 multiaxial system.
Developmental Evaluation
Mrs. Rivera was interviewed about Lucas’ medical and developmental history by a developmental pediatrician. She reported that Lucas is a fraternal twin. Lucas lives with his father, mother, maternal grandmother, and twin brother. Mrs. Rivera and her mother are Lucas’ primary caregivers. However, Lucas’ grandmother finds it challenging to manage Lucas’ behaviors when his mother is not present. Mrs. Rivera reported that she stopped attending church and spending time with friends so that she can be with Lucas.. Her husband, Mr. Rivera, works long hours, which limits the time he spends with Lucas and his brother. Mrs. Rivera stated that she appreciates the opportunity to remain home as the primary caregiver and that the roles she and her husband have in the supporting the family are consistent with their family and cultural values.
Mrs. Rivera stated that she is proficient in English and Spanish. Both languages are spoken at home. However, Mrs. Rivera stated that she has attempted to only speak to Lucas in English after his pediatrician suggested that exposure to both languages may be confusing Lucas and contributing to his speech delay. She reported feeling guilty about not speaking in her native language to Lucas and feeling as though speaking Spanish would help her feel more connected to Lucas. Mrs. Rivera explained that her speaking English creates tension with her husband and mother, and they have continued to speak with Lucas in Spanish. She discussed “familism” (i.e., the importance of solidarity among family members) and explained that she feels responsible for causing tension in family relationships. Mrs. Rivera reported that Lucas does not use words to communicate in either language.
Mrs. Rivera reported a complicated pregnancy with Lucas and his twin, which was her first. Specifically, she reported preeclampsia and severe nausea during pregnancy. She took Zofran during her first 2 months of pregnancy to reduce nausea. Lucas and his brother were born at 35 weeks gestation via vaginal delivery. Lucas weighed 5 pounds, 7 ounces at birth. Lucas remained in the hospital for monitoring for 48 hours, at which time he was discharged.
Mrs. Rivera reported that Lucas attained motor milestones in a timely manner. He sat without support by 6 months, crawled by 9 months, and walked by 13 months. In contrast, his social and language milestones were delayed. At 14 months, Lucas smiled, but rarely pointed, showed objects to his caregivers, or turned to his caregiver when his name was called. With regard to language skills, Lucas babbled but he did not use any words.
Mrs. Rivera also reported that Lucas had difficulty falling and staying asleep most nights. She explained that she values co-sleeping and she has slept with Lucas and his brother in their room since the twins were born. Lucas was described as a “light sleeper” during infancy, but over the 3 months prior to the evaluation he had become increasingly distressed during bedtime. Lucas cried for approximately 1 hour most nights when he was put to sleep and it was difficult to soothe him. Mrs. Rivera reported that Lucas falls asleep more easily in a car and she drove around the neighborhood with Lucas for at least 40 minutes every evening to help him fall asleep. She noted that Lucas sometimes woke when transferred from the car seat to his bed, and he usually had difficulty falling asleep again. Lucas’ grandmother helped Mrs. Rivera with bedtime routines and started co-sleeping with Lucas’ brother. Mrs. Rivera expressed sadness about not being able to co-sleep with Lucas’ brother. She also reported that Lucas’ sleep-related challenges interfered with her and her mother’s sleep and contributed to them feeling tired during the day.
In addition to the interview with Mrs. Rivera, several assessments were administered (see Table 1). Lucas was compliant throughout testing and our observations were corroborated by Ms. Rivera’s reporting; therefore, results are considered an accurate representation of his functioning.
Table 1. Assessments and Results

DC:0–5 emphasizes that young children are embedded within multiple systems that must be considered during evaluation, diagnosis, and treatment planning.
Photo: shutterstock/Rawpixel.com
Bayley-4
Lucas’ scores were corrected for his gestational age. Lucas’ motor skills were developing broadly as expected; he grasped blocks with his hands, transferred a small item from one hand to another, walked with his mother’s support, and stood independently. His cognitive skills were in the low average range; he looked at pictures with interest and searched for an object when it fell to the floor. He did not find blocks hidden under a cup. Lucas’ language skills were markedly delayed and appear to have declined since his 6-month assessment. He sometimes reacted to voices and babbled; he did not respond to his name, recognize words, or use language or gestures to communicate.
Vineland-3
Lucas exhibited significant delays in his communication skills; his receptive language was somewhat more developed than his expressive language. Lucas’ daily living skills were also very low; he did not cooperate actively in bathing or being dressed. Lucas’ socialization fell within the very low range and reflected his lack of interest in other children. Consistent with observations during the Bayley-4, Lucas’ motor skills fell within the average range.
ADOS-2
Lucas demonstrated limited social communication behaviors. During the evaluation, he babbled with a few sounds, whined, and cried periodically, but did not use any words or word approximations. Further, when sharing enjoyment, requesting, or when frustrated he did not pair his vocalizations with eye contact or gestures. For instance, when Lucas wanted the examiner to blow bubbles, he walked toward the bubbles and tried to reach for them himself, never looking or turning to the examiner to enlist her help in any way. Similarly, when he was enjoying placing shapes in a container and the examiner blocked the container, Lucas moved her hand without looking up at her. When verbally prompted with “You do it!”, Lucas imitated the examiner’s functional use of toys, including making a toy frog hop. However, Lucas did not spontaneously demonstrate functional play during free play. He also demonstrated unusual repetitive play and sensory interests throughout the evaluation, including fixating on the light, flicking a doll’s eyelids, running his hand along the bristles of a hairbrush, and spinning a car’s wheels repeatedly.
Dyadic Interaction
The examiner then observed a 15-minute play interaction between Lucas and Mrs. Rivera. The examiner invited Lucas and Mrs. Rivera to play with the toys in the room and to interact as they typically do at home. Lucas and Mrs. Rivera sat facing each other on a play mat. Mrs. Rivera demonstrated positive affect and high responsivity and directiveness.
Consistent with his earlier behavior in the ADOS, Lucas repeatedly flicked a doll’s eyelids, spun the wheels of a toy car, and lined up toy cars along a windowsill. Mrs. Rivera asked Lucas questions and provided several directives to suggest ways to play with the toys functionally (e.g., “make your car drive” “do you want to race?”), but Lucas did not respond or follow her directives. Mrs. Rivera then offered Lucas a snack. Lucas did not respond when his mother asked “Lucas, do you want Cheerios?” but he ate the snack when it was placed in front of him. He whined and walked toward his mother’s bag when he finished his snack; Mrs. Rivera immediately provided more Cheerios.
Interdisciplinary Team Consultation Meeting
Following the evaluation, the interdisciplinary team (consisting of a developmental pediatrician, licensed clinical psychologist, and social worker) working with Lucas and his family met to discuss their impressions and formulate a diagnostic summary and treatment recommendations. After a brief presentation from each provider on Lucas’ family history, health and developmental history, current developmental functioning, social–communication functioning, and behavioral symptomology, there was disagreement among team members regarding whether Lucas should be given a diagnosis of ASD or early atypical ASD, which is a diagnosis for children showing impairment who do not meet full criteria for ASD. The developmental pediatrician stressed that 14 months felt very early to give an ASD diagnosis, especially considering Lucas’ premature birth and his strengths. She wondered about suggesting that the family return to the clinic in 6 months for a re-evaluation. The clinical psychologist supported giving an ASD diagnosis because of Lucas’ developmental risk factors; his clear deficits in social communication, play, language, and adaptive functioning; and his mother’s high levels of concern regarding Lucas’ delays. She noted that Lucas’ language was significantly more delayed at 14 months than it had been at 6 months (a slow regression that is consistent with ASD development; Pearson et al., 2018). Finally, she noted that Latinx children whose primary language is Spanish experience barriers to early diagnosis of ASD due to fewer providers offering developmental screeners in Spanish and families’ difficulty accessing developmental specialists (Zuckerman et al., 2013). Therefore, she advocated for the importance of addressing this diagnostic disparity and diagnosing ASD in young children when symptoms are present.
The team reviewed the DC:0–5 criteria included in the diagnostic algorithm for ASD and came to consensus on a diagnosis based on evidence of each of the social–communication and restrictive and repetitive behavior symptom criteria as well as the presence of impairment. Lucas also demonstrated symptoms consistent with criteria for sleep onset disorder including requiring more than 30 minutes to fall asleep most nights and related impairment to Lucas and his caregivers. (See Table 2.)
Table 2. DC:0-5 Diagnostic Summary
Feedback to Caregivers
Mrs. Rivera attended the feedback meeting alone. The clinician made clear that she could be available to meet with Mrs. Rivera’s husband and mother to discuss the results of the evaluation and the recommendations in Spanish. The team presented their findings to Mrs. Rivera using the DC:0–5 multiaxial framework. This approach provided her with a holistic and comprehensive overview of Lucas’ strengths and areas for further development, especially as it related to the family culture and values.
The clinician provided information about ASD, linked the corresponding behaviors they observed in Lucas (see Table 1), and recommended that Lucas participate in Part C: Early Intervention services. The providers explained that although an ASD diagnosis at 14 months is generally stable, approximately 12–15% of individuals diagnosed before 3 years old lose their diagnosis (Giserman-Kiss & Carter, 2020). The clinician also diagnosed Lucas with sleep onset disorder and reviewed the DC:0–5 criteria for the disorder with Mrs. Rivera (see Table 1). The clinician explained that children with ASD have a high rate of comorbid clinical disorders (Bauman, 2010; Gillberg & Billstedt, 2000), including sleep problems. She summarized the information that Mrs. Rivera shared regarding her preferences for co-sleeping and the ways in which she responds to Lucas’ sleep challenges. The clinician explained that, like Mrs. Rivera, many parents of children with anxiety or sleep-related concerns report high accommodation of their children by changing their behavior or family routines in order to reduce their children’s distress (Chevalier et al., 2021; Thompson-Hollands et al., 2014). Higher accommodation is associated with higher maternal distress and more severe sleep problems in children (Chevalier et al., 2021; Thompson-Hollands et al., 2014). The clinician provided recommendations that honored the family’s co-sleeping preferences and introduced a behavioral therapist to address sleep hygiene, including collaboratively planning for reductions in parental accommodation.

DC:0–5 posits that early relationships are critical to all children’s development. Photo: paulaphoto/shutterstock
Completing an observation of parent–child behavior allowed the clinician to learn about Mrs. Rivera’s strengths, including her high responsivity and engagement. The clinician shared her impression of Mrs. Rivera’s strengths as a caregiver, including that she (1) is attuned to Lucas’ preferences and needs, (2) readily spends time with him and tries to engage him in play and other developmentally appropriate activities, and (3) effectively provides comfort when he is distressed. In addition, she shared information about Lucas’ strengths and interests that were observed, including his strong preference for toy cars. The clinician recommended that Mrs. Rivera enroll in a parent-mediated Naturalistic Developmental Behavioral Intervention in order to leverage her strengths as an involved caregiver. She explained that these interventions are based on developmental and behavioral theory and teach parents to use naturalistic intervention techniques to promote their children’s social communication during play and other daily routines (Dai et al., 2021; Ingersoll & Wainer, 2013). Also, parent-mediated interventions increase the dose of intervention and the generalization because caregivers are able to practice kills with their children throughout the day across a variety of contexts (Sachse & Von Suchodoletz, 2008). The clinician informed Mrs. Rivera that by participating in a parent-mediated intervention (e.g., JASPER, Goods et al., 2013; Project Impact, Ingersoll & Wainer, 2013), she will learn to imitate Lucas’ play in order to make play interactive, and then to introduce new ways of playing and elaborate on play routines that Lucas enjoys in order to encourage Lucas’ increased flexibility and functional play. Mrs. Rivera will also be taught prompting and reinforcement strategies to encourage Lucas’ functional use of language and social communication.
Further, the clinician noted high levels of family stress, especially surrounding Lucas’ lack of social engagement and sleep issues, as well as in relation to his caregivers’ differing views of his current functioning and needs. The clinician acknowledged that raising a child with ASD can increase stress in and between caregivers, particularly given the caregivers’ lack of consensus about Lucas’ development. The team requested Mrs. Rivera’s permission to arrange a meeting with Mr. Rivera (either alone or with Mrs. Rivera) to explain the ASD diagnosis and support his view that using Spanish in the home was appropriate. Specifically, the clinician explained that bilingual caregivers of children with ASD often believe that learning more than one language is deleterious for their children’s language development, and this notion is often corroborated by providers (Bird et al., 2016; Ijalba, 2016). In most cases, caregivers opt to speak to their children in the culture-dominant language, even when this language is not the caregiver’s native or proficient language (Hampton et al., 2017; Kremer-Sadlik, 2005; Yu, 2013), just as she did. The clinician emphasized that this decision has negative consequences for children and their families. For example, children are often exposed to less language at home if the caregivers are not communicating with their child in their dominant language (Altan & Hoff, 2018; Place & Hoff, 2011) and caregivers frequently report reductions in the quality of parent–child interactions when they are not communicating in their native language. The clinician noted ways in which these reductions can cascade into greater social communication impairments in children with ASD (Beauchamp & MacLeod, 2017; Charman, 2003; Kremer-Sadlik, 2005). Finally, the clinician normalized that many caregivers express sadness when they feel as though they cannot speak with their children in their native language and they report that communication feels more strained when they speak in a nondominant language (Hampton et al., 2017; Yu, 2013). The clinician stated that despite the pervasive notion that dual language exposure contributes to language delays in children with ASD, there is no empirical evidence to support this claim. In fact, research has documented that being exposed to one versus two languages does not influence the age at which language milestones are attained nor overall language skills in children with ASD (Beauchamp & MacLeod, 2017; Dai et al., 2018; Drysdale et al., 2015; Ohashi et al., 2012; Petersen et al., 2012; Valicenti-McDermott et al., 2013). The clinician shared her hope that she could engage Mr. Rivera in supporting Lucas’ language acquisition by continuing to speak with him in both languages and by framing the recommended interventions as the supports that Lucas would need to have the best chance of catching up versus losing further ground. The clinician conveyed her hope that Mrs. Rivera’s confidence in resuming to speak with Lucas in both Spanish and English would reduce tension with her husband and mother and increase familism, thereby increasing her emotional well-being. Finally, the clinician normalized that caregivers often experience a variety of feelings when their child receives a diagnosis of autism and caregivers may have different strategies to cope with these feelings. Mrs. Rivera was encouraged to initially share the diagnosis only with people who would be supportive of her, allowing her time to process this information.
Last, the clinician explained that children who have a first-degree relative with ASD are more likely to have symptoms of ASD (Messinger et al., 2013; Ozonoff et al., 2011). Heritability for ASD is even higher for male fraternal twins, with heritability ranging from 31–40% (Ronald & Hoekstra, 2011; Rosenberg et al., 2009). Therefore, the clinician noted that it is fortunate that Lucas’ twin is being monitored by the infant development follow-up clinic. She recommended that Mrs. Rivera continue to attend follow-up appointments with both Lucas and his brother.

As physical, neurodevelopmental, and mental health are interrelated, Axis III provides a framework for considering the impact of a child’s physical health on clinical symptoms. Photo: GOLFX/shutterstock
Conclusion
DC:0–5 provided a framework for Lucas’ providers to gather information about his overall functioning and to consider the sociocultural and familial environment in which he is being raised. This holistic approach allowed providers to learn about the factors that impacted Lucas’ mental health, development, and family well-being, and to tailor recommendations accordingly.
Author Bios
Yael Dai, PhD, is a postdoctoral research fellow in the Psychology Department at the University of Massachusetts Boston. She received her doctorate in clinical psychology from the University of Connecticut and completed her predoctoral internship at Kennedy Krieger Institute. Dr. Dai is interested in the development, evaluation, and implementation of interventions for children with autism and their families. Her research also focuses on promoting early identification of autism, increasing access to interventions, and treating anxiety.
Daina M. Tagavi, PhD, is a postdoctoral research fellow in the Department of Psychology at the University of Washington. Dr. Tagavi completed her bachelor’s degree at Pepperdine University and her master’s degree in psychology at Boston University. She received her doctorate in clinical psychology from the University of California, Santa Barbara and completed her predoctoral internship at the University of Washington and Seattle Children’s Hospital. Her research focuses on the development, adaptation, dissemination, and implementation of assessments and interventions for individuals with ASD.
Alice S. Carter, PhD, is a professor in the Psychology Department at the University of Massachusetts Boston. She received her doctorate in clinical psychology from he University of Houston and completed her predoctoral internship and a postdoctoral fellowship at the Yale Child Study Center. Her work focuses on early identification of infant mental health and neurodevelopmental disorders, addressing health disparities in access to evidence-based services, and evaluating community-based interventions.
Suggested Citation
Dai, Y., Tagavi, D. M., & Carter, A. S., (2021). Replacing a spotlight with a lantern: Using the DC:0–5 multiaxial framework when diagnosing autism spectrum disorder in early childhood. ZERO TO THREE Journal, 42(2), 20–29.
References
Altan, A., & Hoff, E. (2018). Complex structures in the child-directed speech of native and nonnative speakers. In D. Buğa, & M. Coşgun Ögeyik (Eds.), Psycholinguistics and cognition in language processing (pp. 127–139). IGI Global.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
Anderson, D. K., Liang, J. W., & Lord, C. (2014). Predicting young adult outcome among more and less cognitively able individuals with autism spectrum disorders. Journal of Child Psychology and Psychiatry, 55(5), 485–494.
Baker, J. K., Seltzer, M. M., & Greenberg, J. S. (2011). Longitudinal effects of adaptability on behavior problems and maternal depression in families of adolescents with autism. Journal of Family Psychology, 25(4), 601–609.
Bauman, M. L. (2010). Medical comorbidities in autism: Challenges to diagnosis and treatment. Neurotherapeutics, 7(3), 320–327.
Bayley, N., Bayley, N., & Aylward, G. (2019). Bayley scales of infant and toddler development, (4th ed.). NCS Pearson.
Beauchamp, M. L., & MacLeod, A. A. (2017). Bilingualism in children with autism spectrum disorder: Making evidence based recommendations. Canadian Psychology, 58(3), 250–262.
Bird, E. K. R., Genesee, F., & Verhoeven, L. (2016). Bilingualism in children with developmental disorders: A narrative review. Journal of Communication Disorders, 63, 1–14.
Charman, T. (2003). Why is joint attention a pivotal skill in autism? Philosophical Transactions of the Royal Society of London. Series B: Biological Sciences, 358(1430), 315–324.
Chevalier, L. L., O’Connor, E. E., Holly, L. E., Langer, D. A., & Pincus, D. B. (2021). The relationship between parental accommodation and sleep-related problems in children with anxiety. Journal of Developmental & Behavioral Pediatrics, 42(2), 114–121.
Dai, Y. G., Burke, J. D., Naigles, L., Eigsti, I. M., & Fein, D. A. (2018). Language abilities in monolingual- and bilingual-exposed children with autism or other developmental disorders. Research in Autism Spectrum Disorders, 55, 38–49.
Dai, Y. G., Thomas, R. P., Brennan, L., Helt, M. S., Barton, M. L., Dumont- Mathieu, T., & Fein, D. A. (2021). Development and acceptability of a new program for caregivers of children with autism spectrum disorder: Online parent training in early behavioral intervention. Journal of Autism and Developmental Disorders, 51, 4166–4185.
Drysdale, H., van der Meer, L., & Kagohara, D. (2015). Children with autism spectrum disorder from bilingual families: A systematic review. Review Journal of Autism and Developmental Disorders, 2(1), 26–38.
Gillberg, C., & Billstedt, E. (2000). Autism and Asperger syndrome: Coexistence with other clinical disorders. Acta Psychiatrica Scandinavica, 102(5), 321–330.
Giserman-Kiss, I., & Carter, A. S. (2020). Stability of autism spectrum disorder in young children with diverse backgrounds. Journal of Autism and Developmental Disorders, 50(9), 3263–3275. https://doi.org/10.1007/s10803-019-04138-2
Goods, K. S., Ishijima, E., Chang, Y. C., & Kasari, C. (2013). Preschool based JASPER intervention in minimally verbal children with autism: Pilot RCT. Journal of Autism and Developmental Disorders, 43(5), 1050–1056.
Hampton, S., Rabagliati, H., Sorace, A., & Fletcher-Watson, S. (2017). Autism and bilingualism: A qualitative interview study of parents’ perspectives and experiences. Journal of Speech, Language, and Hearing Research, 60(2), 435–446.
Hartley, S. L., DaWalt, L. S., & Schultz, H. M. (2017). Daily couple experiences and parent affect in families of children with versus without autism. Journal of Autism and Developmental Disorders, 47(6), 1645–1658.
Ijalba, E. (2016). Hispanic immigrant mothers of young children with autism spectrum disorders: How do they understand and cope with autism? American Journal of Speech-Language Pathology, 25(2), 200–213.
Ingersoll, B., & Gergans, S. (2007). The effect of a parent-implemented imitation intervention on spontaneous imitation skills in young children with autism. Research in Developmental Disabilities, 28(2), 163–175.
Ingersoll, B., & Wainer, A. (2013). Initial efficacy of Project ImPACT: A parent- mediated social communication intervention for young children with ASD. Journal of Autism and Developmental Disorders, 43(12), 2943–2952.
Karst, J. S., & Van Hecke, A. V. (2012). Parent and family impact of autism spectrum disorders: A review and proposed model for intervention evaluation. Clinical Child and Family Psychology Review, 15(3), 247–277.
Kremer-Sadlik, T. (2005). To be or not to be bilingual: Autistic children from multilingual families. In J. Cohen, K. T. McAlister, K. Rolstad, & J. MacSwan (Eds.), Proceedings of the 4th International Symposium on Bilingualism (pp. 1225–1234). University of Arizona, United States.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Leventhal, B. L., DiLavore, P. C., ... & Rutter, M. (2000). The Autism Diagnostic Observation Schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30(3), 205–223.
MacDonald, R., Parry-Cruwys, D., Dupere, S., & Ahearn, W. (2014). Assessing progress and outcome of early intensive behavioral intervention for toddlers with autism. Research in Developmental Disabilities, 35(12), 3632–3644.
Magaña, S., Lopez, K., Aguinaga, A., & Morton, H. (2013). Access to diagnosis and treatment services among Latino children with autism spectrum disorders. Intellectual and Developmental Disabilities, 51(3), 141–153.
Mandell, D. S., Listerud, J., Levy, S. E., & Pinto-Martin, J. A. (2002). Race differences in the age at diagnosis among Medicaid-eligible children with autism. Journal of the American Academy of Child & Adolescent Psychiatry, 41(12), 1447–1453.
Mandell, D. S., Novak, M. M., & Zubritsky, C. D. (2005). Factors associated with age of diagnosis among children with autism spectrum disorders. Pediatrics, 116(6), 1480–1486.
Mandell, D. S., Xie, M., Morales, K., Lawer, L., McCarthy, M., & Marcus, S. C. (2011). The interplay of outpatient services and psychiatric hospitalization among Medicaid-enrolled children with autism spectrum disorders. Archives of Pediatric and Adolescent Medicine, 166(1), 68–73.
Martínez-Pedraza, F. D. L., & Carter, A. S. (2009). Autism spectrum disorders in young children. Child and Adolescent Psychiatric Clinics, 18(3), 645–663.
Mazzoni, S., Veronesi, C., Vismara, L., Laghi, F., & Phillipp, D. (2018). Family coordination in families who have a child with autism spectrum disorder. Journal of Child and Family Studies, 27(10), 3107–3116.
McHale, J. P., & Rasmussen, J. L. (1998). Coparental and family group-level dynamics during infancy: Early family precursors of child and family functioning during preschool. Development and Psychopathology, 10(1), 39–59.
Messinger, D., Young, G. S., Ozonoff, S., Dobkins, K., Carter, A., Zwaigenbaum, L., ... & Sigman, M. (2013). Beyond autism: A Baby Siblings Research Consortium study of high- risk children at three years of age. Journal of the American Academy of Child & Adolescent Psychiatry, 52(3), 300–308.
Muskens, J. B., Velders, F. P., & Staal, W. G. (2017). Medical comorbidities in children and adolescents with autism spectrum disorders and attention deficit hyperactivity disorders: A systematic review. European Child & Adolescent Psychiatry, 26(9), 1093–1103.
Ohashi, J. K., Mirenda, P., Marinova-Todd, S., Hambly, C., Fombonne, E., Szatmari, P., ... & Pathways in ASD Study Team. (2012). Comparing early language development in monolingual-and bilingual-exposed young children with autism spectrum disorders. Research in Autism Spectrum Disorders, 6(2), 890–897.
Orinstein, A. J., Suh, J., Porter, K., De Yoe, K. A., Tyson, K. E., Troyb, E., ... & Fein, D. A. (2015). Social function and communication in optimal outcome children and adolescents with an autism history on structured test measures. Journal of Autism and Developmental Disorders, 45(8), 2443–2463.
Ozonoff, S., Young, G. S., Carter, A., Messinger, D., Yirmiya, N., Zwaigenbaum, L., ... & Stone., W. L. (2011). Recurrence risk for autism spectrum disorders: A Baby Siblings Research Consortium study. Pediatrics, 128(3), e488–e495.
Pearson, N., Charman, T., Happé, F., Bolton, P. F., & McEwen, F. S. (2018). Regression in autism spectrum disorder: Reconciling findings from retrospective and prospective research. Autism Research, 11(12), 1602–1620.
Petersen, J. M., Marinova-Todd, S. H., & Mirenda, P. (2012). Brief report: An exploratory study of lexical skills in bilingual children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 42(7), 1499–1503.
Pierce, K., Gazestani, V. H., Bacon, E., Barnes, C. C., Cha, D., Nalabolu, S., ... Courchesne, E. (2019). Evaluation of the diagnostic stability of the early autism spectrum disorder phenotype in the general population starting at 12 months. JAMA Pediatrics, 173(6), 578–587.
Place, S., & Hoff, E. (2011). Properties of dual language exposure that influence 2-year-olds’ bilingual proficiency. Child Development, 82(6), 1834–1849.
Rogers, S. J., & Vismara, L. A. (2008). Evidence-based comprehensive treatments for early autism. Journal of Clinical Child & Adolescent Psychology, 37(1), 8–38.
Rogers, S. J., Vismara, L., Wagner, A. L., McCormick, C., Young, G., & Ozonoff, S. (2014). Autism treatment in the first year of life: A pilot study of infant start, a parent-implemented intervention for symptomatic infants. Journal of Autism and Developmental Disorders, 44(12), 2981–2995.
Ronald, A., & Hoekstra, R. A. (2011). Autism spectrum disorders and autistic traits: A decade of new twin studies. American Journal of Medical Genetics Part B: Neuropsychiatric Genetics, 156(3), 255–274.
Rosenberg, R. E., Law, J. K., Yenokyan, G., McGready, J., Kaufmann, W. E., & Law, P. A., (2009). Characteristics and concordance of autism spectrum disorders among 277 twin pairs. Archives of Pediatric and Adolescent Medicine, 163, 907–914.
Sachse, S., & Von Suchodoletz, W. (2008). Early identification of language delay by direct language assessment or parent report? Journal of Developmental & Behavioral Pediatrics, 29(1), 34–41.
Sarche, M., Tsethlikai, M., Godoy, L., Emde, R., & Fleming, C. M. (2019). Cultural perspectives for assessing infants and young children. In R. DelCarmen- Wiggins & A. S. Carter (Eds.), The Oxford handbook of infant, toddler, and preschool mental health assessment (2 ed., pp. 9–28). Oxford University Press.
Schuck, R. K., Tagavi, D. M., Penner-Baiden, K. M.., Dwyer, P., Williams, Z. J., Osuna, A., Ferguson, E. F., Jimenez Munoz, M., Poyser, S., Johnson, J. F., Vernon, T. W. (2021). Neurodiversity and autism intervention: Reconciling perspectives through a Naturalistic Developmental Behavioral Intervention framework. Journal of Autism and Developmental Disorders. Advanced Online Publication: https://doi.org/10.1007/s10803-021-05316-x
Serrata, C. A. (2012). Psychosocial aspects of parenting a child with autism. Journal of Applied Rehabilitation Counseling, 43(4), 29–35.
Siller, M., & Sigman, M. (2002). The behaviors of parents of children with autism predict the subsequent development of their children’s communication. Journal of Autism and Developmental Disorders, 32(2), 77–89.
Sparrow, S. S., Cicchetti, D. V., & Saulnier, C. A. (2016). Vineland-3: Vineland adaptive behavior scales. Psychcorp
Thompson-Hollands, J., Kerns, C. E., Pincus, D. B., & Comer, J. S. (2014). Parental accommodation of child anxiety and related symptoms: Range, impact, and correlates. Journal of Anxiety Disorders, 28(8), 765–773.
Valicenti-McDermott, M., Tarshis, N., Schouls, M., Galdston, M., Hottinger, K., Seijo, R., ... & Shinnar, S. (2013). Language differences between monolingual English and bilingual English-Spanish young children with autism spectrum disorders. Journal of Child Neurology, 28(7), 945–948.
Webb, S. J., & Jones, E. J. (2009). Early identification of autism: Early characteristics, onset of symptoms, and diagnostic stability. Infants and Young Children, 22(2), 100–118.
Yu, B. (2013). Issues in bilingualism and heritage language maintenance: Perspectives of minority-language mothers of children with autism spectrum disorders. American Journal of Speech-Language Pathology, 22(1), 10–24.
ZERO TO THREE. (2016). DC:0–5TM: Diagnostic classification of mental health and developmental disorders in infancy and early childhood (DC:0–5).
Zuckerman, K. E., Mattox, K., Donelan, K., Batbayar, O., Baghaee, A., & Bethell, C. (2013). Pediatrician identification of Latino children at risk for autism spectrum disorder. Pediatrics, 132(3), 445–453.