Angela J. Narayan, Victoria M. Atzl, Jillian S. Merrick, and Laura M. River, University of Denver
Rachel Peña, Denver Health & Hospital Authority, Denver, Colorado
Abstract
Clinical research during the pregnancy period is maximally beneficial for participants if it is positive, inclusive, and therapeutic. We describe our ongoing study of ethnically diverse, low-income pregnant women and fathers-to-be that leverages participants’ benevolent childhood experiences (BCEs) and promotes insight to counteract mental health and relationship problems before babies are born. Although many participants report extensive childhood trauma, cumulative stress, and elevated depression and posttraumatic stress disorder (PTSD) symptoms, most also report high levels of BCEs, which show promising associations with well-being. Participant reflections at the end of the study illustrate that they feel their stories are valued, learn to connect past experiences to present functioning, gain insights about their romantic relationships, and enjoy the research experience.
Although the pregnancy period is often joyful and hopeful, it can also be a complicated transition marked by heightened psychological distress, particularly for individuals with childhood trauma. For women with histories of childhood maltreatment and other dysfunction in their families of origin, a pregnancy may summon emotions and memories of negative and abusive caregiving, leading to heightened symptomatology. Indeed, pregnant women often have higher rates of posttraumatic stress disorder (PTSD) than their non-pregnant counterparts with similar trauma histories, in part because becoming pregnant may evoke recollections of unresolved childhood trauma as women consider the type of mothers they want to be (Seng et al., 2010).
Because pregnancy elicits reflection on one’s childhood, it also represents an important window to build insight and foster resilience. Many pregnant women intentionally consider how to avoid falling into the dysfunctional or abusive patterns of their parents and instead draw on childhood experiences of love and kindness as templates to re-create in the next generation (Slade & Cohen, 1996; Sperlich & Seng, 2008). In this way, the pregnancy period is a double-edged sword, during which trauma-related distress and hopeful optimism co-exist to portend both risk and resilience for the mother and the new baby.
Research studies and clinical practices that harness resilience processes for pregnant women with childhood trauma are scarce. A recent systematic review found only 18 empirical studies that identified promotive or protective factors to buffer against effects of childhood trauma on the well-being of pregnant women and their infants (Atzl, Grande, Davis, & Narayan, 2019). Further, rather than assessing and leveraging women’s strengths, coping strategies, and resources, most routine prenatal care only screens for current distress and stressors that may harm the woman or fetus, such as prenatal depression symptoms or the presence of intimate partner violence victimization. To date, uncovering resilience processes among pregnant women with trauma histories has not been a priority, but it is key to promoting better outcomes for families during the pregnancy period and beyond.
In 2015 in San Francisco, CA, we conducted an empirical study using a trauma-informed model of clinical research, combined with therapeutic assessment of risk and resilience during pregnancy (Narayan et al., 2017). This study gathered rich data while simultaneously affording participants opportunities to reflect on strengths in addition to stressors, become more intentional about their plans for parenthood, and connect with referrals for mental health care and concrete needs. In this context, women felt comfortable disclosing very high levels of contemporaneous and childhood trauma, and they expressed gratitude that they had participated and shared their stories.
Major insights from the San Francisco study included the need—for us as researchers and for pregnant women—to not only focus on hardships, but to draw upon assets and resources during pregnancy. Indeed, the first empirical report from that study documented that pregnant women with higher levels of benevolent childhood experiences (BCEs), which are individual, relational, and contextual supports and resources, had lower PTSD symptoms and exposure to fewer stressful life events during pregnancy, even if they had extensive childhood trauma (Narayan, Rivera, Bernstein, Harris, & Lieberman, 2018).
In this article, we describe the success of this trauma-informed, therapeutic research model in a separate sample of pregnant women from Denver, CO, and emphasize that the benefits of therapeutic assessment during pregnancy can also extend to low-income, ethnically diverse fathers expecting a baby. Fathers-to-be, particularly those with childhood trauma histories, are vastly unrecognized as needing resources to support their resilience during the transition to fatherhood, yet they make up half of the caregiving equation (Cabrera, Karberg, & Kuhns, 2017; Lee, Knauer, Lee, MacEachern, & Garfield, 2018). Moreover, unresolved experiences of childhood maltreatment and other interpersonal trauma are likely to similarly haunt men and threaten their psychological well-being as they consider their identities as fathers either for the first time or for a new addition to the family. More attention is needed to help fathers share and recover from their trauma histories, particularly during the vulnerable yet hopeful period when they are expecting a baby (Astone & Peters, 2014). The aims of this report are to
- describe the life experiences and mental health of the first 101 pregnant women of the 200 we plan to enroll in Denver, in comparison to (a) 101 pregnant women from San Francisco and (b) 72 fathers-to-be from Denver;
- highlight promotive effects of BCEs in fathers-to-be compared to pregnant women; and
- share the reflections of participating families in trauma-informed, resilience-based perinatal research.
Of note, we refer to the pregnant participants as women and their partners as men/fathers-to-be because that is how the vast majority of participants identified, but we recognize that this may not align with all gender identities and family structures.
Study Design and Sample
The eligibility criteria in Denver are identical to the criteria used in San Francisco (Narayan et al., 2017), with the exception that in San Francisco we also included Spanish-speaking women (because we had Spanish-speaking research personnel). In both cities, women were recruited from the metro county’s general hospital (Denver Health or Zuckerberg San Francisco General Hospital), which serves the majority of individuals receiving public health insurance or who are medically uninsured. Women were recruited from prenatal appointments at each hospital’s obstetrics/gynecology department and childbirth classes, as well as at community clinics and agencies serving pregnant women. Eligibility criteria for both studies were that women were in their second or third trimester (to allow for ample time to reflect on being pregnant), were planning to deliver at the general hospital, were at least 18 years old, and spoke English (or Spanish in San Francisco). In Denver, we are also recruiting fathers-to-be who are at least 18 years old and English-speaking. Fathers are specifically recruited through online classified advertising sites and parenting classes for fathers-to-be.
Similar to San Francisco, all Denver participants complete a clinical research protocol on mental health symptoms, childhood trauma and life stressors, BCEs, relationship dynamics, and demographic information. All questions are read aloud to minimize differences in reading or language ability, and to facilitate a supportive dialogue. Participants also provide narratives that encourage them to reflect on topics such as attributions toward their partner and baby in utero, how they plan to parent as compared to their own mother or father, and what aspects of their lives are currently the most fulfilling and joyful, versus difficult and stressful. These open-ended questions are administered early in the protocol to facilitate rapport for many women and men who have never participated in research and to allow participants to share meaningful experiences via a flexible and validating conversation. If both partners complete the study interview during the same appointment, they also identify together and discuss one of the biggest problems in their relationship for several minutes, and conclude by talking to each other about a positive life event (Salvatore, Kuo, Steele, Simpson, & Collins, 2011).
Recruitment Lessons Learned
Of 102 families who have participated in Denver thus far, 71% have included both parents. Denver data presented below reflects 101 pregnant women and 72 fathers-to-be (one family included a father-to-be, but the pregnant woman did not participate). For the 30 families in which only the pregnant woman participated, fathers-to-be did not participate because they were too busy with work (n = 14), were completely uninvolved with and unsupportive of the pregnancy (n = 9), were currently incarcerated or on house-arrest (n = 3), or the pregnant women reported not having any contact with them because of recent and severe intimate partner violence (n = 4). In more than one quarter (26%, n = 19) of the 72 families in which both parents participated, the father-to-be made initial contact to enroll in the study. These numbers are in stark contrast to those in San Francisco, where fathers-to-be were not directly recruited and only 14 of 101 participated. In San Francisco, pregnant women often “spoke for” the fathers, saying that they were too busy or would not want to do the study. These low participation rates are even more surprising considering the vast majority (75%) of San Francisco women were romantically involved with the baby’s father at the time of the study. In reality, when directly given the opportunity, most fathers-to-be seem to want to participate or have concrete reasons for being unable to do so.
Measures and Comparison Data on Pregnant Women
We present data collected in Denver on both parents’ demographics, reproductive history, BCEs, Adverse Childhood Experiences (ACEs; Centers for Disease Control and Prevention CDC], 2016) and additional lifetime adversities, and current mental health symptoms, all of which are summarized in comparison to pregnant women from San Francisco (Tables 1 and 2; see p. 46 and p. 47).

Fathers-to-be, particularly those with childhood trauma histories, are vastly unrecognized as needing resources to support their resilience during the transition to fatherhood.
Demographics
Pregnant women in both cities were primarily Latina, White, and African-American. Latina women represented the largest group in San Francisco (37%, versus 22% African-American and 20% White), whereas White women currently represent the largest group in Denver (35%, versus 21% African-American and 20% Latina). A greater percentage of women from San Francisco were currently unemployed (67% versus 52% in Denver), although women in both samples had an average educational attainment of a high school degree.
Reproductive History
Across samples, women’s pregnancy histories are strikingly similar. This was the first pregnancy for only approximately 20% of women from both cities, and women had comparable numbers of total pregnancies (about three) and average age at first pregnancy (approximately 20–21 years). In addition, both samples had very similar percentages of women who became pregnant for the first time as teenagers (46% in Denver and 47% in San Francisco). These observations are especially noteworthy because both studies used the same broad eligibility criteria, so similarities suggest that many pregnant women drawn from these cities’ general hospitals may experience comparable demographic and reproductive risks. However, women from Denver were less likely to report that their current pregnancy was unplanned (54% versus 62%), yet were more likely to report that they had ever become pregnant when they did not want to be (lifetime unwanted pregnancy; 52% versus 44%).
Table 1. Participants’ Ratings of Learning Module Elements
BCEs
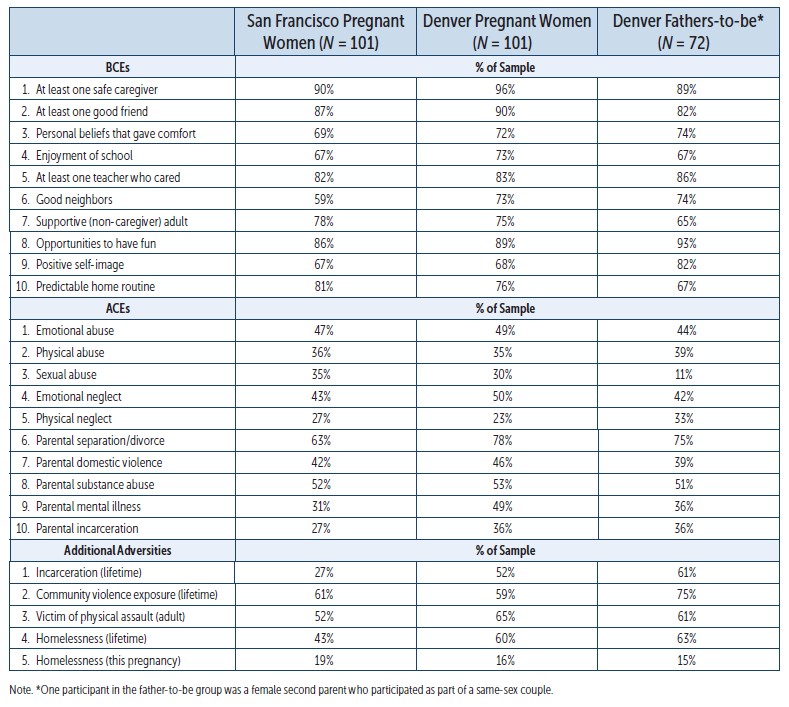
The BCEs scale, developed as a culturally sensitive counterpart to the ACEs scale (CDC, 2016) and available in several languages, is a brief 10-item index of childhood resources (Narayan et al., 2018). Similar to the ACEs scale, positively endorsed items are summed for a total BCEs score. Across samples, women’s mean levels of BCEs were very similar at approximately 8 total. The most apparent difference across samples was that a substantially greater percentage of women from Denver reported growing up with good neighbors (73% versus 59%, Table 2). This discrepancy may reflect the persistence and pervasiveness of homelessness and substance use problems that have characterized San Francisco since the 1980s (Fagan, 2016).
Childhood and Lifetime Adversities
To assess childhood adversity, we used the ACEs scale (CDC, 2016), which includes 10 items indexing five subtypes of childhood maltreatment (emotional, physical, and sexual abuse; and emotional and physical neglect) and five types of family dysfunction (parental divorce/separation, domestic violence, substance use, mental illness, and incarceration). Subscales for maltreatment versus family dysfunction are calculated in addition to the total score (Atzl, Narayan, Rivera, & Lieberman, 2019). Across both samples, pregnant women’s mean levels of total ACEs were comparable (approximately 4 total), as were mean levels of their total childhood maltreatment (women experienced two subtypes on average) and individual maltreatment subtypes (although San Francisco women reported slightly higher rates of childhood sexual abuse, 35% versus 30%, and Denver women reported higher rates of emotional neglect, 50% versus 43%). While mean levels of pregnant women’s total childhood exposure to family dysfunction were also similar (approximately two types on average), Denver women reported higher rates of parental separation/divorce (78% versus 63%), mental illness (49% versus 31%), and incarceration (36% versus 27%).
Pregnant women from both cities reported on several additional adversities (Table 2). Denver women reported substantially higher rates of incarceration (52% versus 27%), and physically victimization by a romantic partner or stranger during adulthood (65% versus 52%), as well as lifetime homelessness (60% versus 43%). However, Denver women reported slightly lower rates of homelessness during the current pregnancy (16% versus 19%).
Table 2. Frequencies of Benevolent Childhood Experiences (BCEs), Adverse Childhood Experiences (ACEs), and Additional Adversities

Determining the best strategies to support expectant fathers’ mental health and coping ability during pregnancy, before stressors affect co-parenting and father–infant relationships, is a priority. Photo: pixelheadphoto digitalskillet/shutterstock
Prenatal Mental Health Problems
All participants were administered the Edinburgh Postnatal Depression Scale (EPDS; Cox, Holden, & Sagovsky, 1987), validated for use with women and men (Ramchandani, Stein, Evans, O’Connor, & ALSPAC Study Team, 2005). The EPDS is a 10-item checklist that assesses depressive symptoms over the past week not solely accounted for by pregnancy symptoms. In Denver, 33% of pregnant women endorsed clinical levels of depression symptoms, compared to 46% of pregnant women in San Francisco (total EPDS score ≥ 10; Earls, 2010).
All participants also completed the PTSD Checklist for DSM-5 (PCL-5: Weathers et al., 2013), a 20-item checklist of PTSD symptoms over the past month. In Denver, 24% of women reported clinical levels of PTSD symptoms, compared to 29% of San Francisco women (total PCL-5 score ≥ 33; National Center for PTSD, 2016).
In general, lower rates of clinical-level mental health symptoms, and particularly lower depression in Denver women, are striking given their higher rates of incarceration, adulthood victimization, and lifetime homelessness. Perhaps Denver women report lower current depression and PTSD symptoms because they are more likely to be currently romantically partnered with their baby’s father (89% versus 75%). Indeed, being romantically partnered with the baby’s father is associated with lower levels of both depression and PTSD symptoms during pregnancy (River, Narayan, Atzl, Rivera, & Lieberman, 2019 ).
Experiences of Fathers-to-Be
Fathers-to-be who participated in Denver are also ethnically diverse, with the highest proportion identifying as White (31%), followed by African-American (26%) and biracial/multiracial (22%). They have comparable average educational attainment (a high-school degree) to both samples of pregnant women, but lower rates of current unemployment (18%).
Pregnancy Risks
Several pregnancy-related risks speak to the need to address men’s role in family planning. On average, men reported being of similar age to both samples of women when a pregnancy first occurred (approximately 22 years old), and approximately one third (36%) of fathers-to-be reported they had been teenagers when a partner first became pregnant. Men who are teenagers when a partner becomes pregnant are at elevated risk of mental health problems, delinquent behavior, and romantic relationship dissolution, which together increase risk of fatherhood absence (Bunting & McAuley, 2004). These cascading consequences further propagate intergenerational dysfunction as daughters of absent fathers are much more likely to engage in premature sexual activity and become pregnant as teenagers (Ellis et al., 2003).
In addition, more than half of fathers-to-be (51%) reported that the current pregnancy was unplanned. Although there is little research about fathers’ perspectives on unplanned or unintended pregnancies, some research suggests that men who perceive the pregnancy as unplanned are more likely to feel stressed and powerless (Clinton & Kelber, 1993). Determining the best strategies to support expectant fathers’ mental health and coping ability during pregnancy, before stressors affect co-parenting and father–infant relationships, is a priority.
Childhood Adversity and Mental Health Problems
Fathers’ mean levels of total ACEs (approximately 4 total) were remarkably similar to both samples of women, as were fathers’ average levels of childhood maltreatment and exposure to family dysfunction (approximately 2 experiences total for each). These findings emphasize that many low-income, underserved men preparing to have a child have significant trauma histories, yet virtually no research has examined how childhood adversity affects men’s mental health during the critical window before babies are born (Astone & Peters, 2014). Moreover, fathers’ rates of individual ACEs were just as high as in both samples of pregnant women, except that men reported lower rates of childhood sexual abuse (11% versus 30–35% in pregnant women) and higher rates of physical neglect (33% versus 23–27% in pregnant women).
Society often expects low-income men to be stable and involved as fathers, despite many having grown up with few resources, low educational attainment, and significant—and unresolved—trauma histories, often including abuse and neglect perpetrated by their caregivers (Settersten & Cancel-Tirado, 2010). We also observed that men reported other adversities at comparable rates to pregnant women, including physical assault victimization by a romantic partner or stranger during adulthood (61% versus 52–65%) and lifetime homelessness (63% versus 43–60%). These accumulating vulnerabilities, combined with feelings of stress and powerlessness following unplanned pregnancies (which peak between 18–25 years old; Finer & Zolna, 2011) make men particularly in need of supportive resources to help deter intergenerational cycles of trauma, poverty, and teen pregnancy. Moreover, research has shown that fathers’ depression symptoms often rise following children’s births through 5 years old (Garfield et al., 2014), further underscoring the urgent need to intervene with fathers during the pregnancy period. Here, we observed that more than one quarter of fathers-to-be (26%) endorsed clinical levels of depression, even before their babies were born.
Descriptive Rates of BCEs
On the bright side, fathers-to-be reported high levels of total BCEs (approximately 8 total), comparable to pregnant women from both cities. Reports of individual BCEs also indicate that fathers-to-be had a high frequency of positive childhood relationships and other resources. For instance, more than 80% of fathers-to-be reported that during at least some part of childhood, they had a caregiver with whom they felt safe, a good friend, a teacher who cared, and opportunities to have fun. Notably, a substantially greater proportion of fathers-to-be reported having a positive self-image during childhood (82%) than both samples of women (67–68%), suggesting many low-income men experience childhood self-esteem as an asset. Alternatively, however, compared to pregnant women, fathers-to-be less frequently reported that they had childhoods with predictable home routines (67% versus 76–81%), consistent with their higher rates of childhood physical neglect, and were less likely to report having a non-caregiver adult who was supportive (65% versus 75–78%).
Promotive Effects of BCEs
This is the first study to provide data, although preliminary, on promotive effects of BCEs on the well-being in fathers-to-be. In the first 72 fathers we have interviewed, higher levels of their BCEs are significantly associated with lower levels of their depression (r = -.32, p < .01) and PTSD symptoms (r = -.31, p < .01), whereas higher levels of Denver pregnant women’s BCEs are only significantly correlated with lower PTSD (but not depression) symptoms (r = -.27, p < .01). For both men and women in Denver, higher levels of total BCEs are only moderately associated with lower levels of total ACEs (r = -.39 and r = -.36, respectively, p < .01 for both). These modest associations between BCEs and ACEs replicate published findings in the San Francisco sample that experiencing maltreatment or family dysfunction does not preclude the presence of supportive resources (Narayan et al., 2018).
Differences between men and women emerged when examining the predictive strength of ACEs versus BCEs. For pregnant women in both cities, higher levels of BCEs significantly predicted lower levels of PTSD symptoms during pregnancy, even after accounting for total ACEs (which were also significant predictors) and demographic covariates (women’s age and gestational age, educational attainment, and primiparous versus multiparous status). These results suggest that the levels of women’s BCEs and ACEs independently affect their level of PTSD symptoms during pregnancy (Narayan et al., 2018). For fathers-to-be, however, only their ACEs predicted mental health during pregnancy. After accounting for fathers’ age and educational level, higher levels of their ACEs, but not lower levels of their BCEs, predicted higher levels of PTSD and depression symptoms during the pregnancy period.

For women, the pregnancy period is filled with change and reorganization at several levels—physical, hormonal, and psychological. Photo: Kl Petro/shutterstock
Although tentative and warranting re-examination when the full sample of 200 families are enrolled in Denver, current findings suggest that, after accounting for ACEs, BCEs may vary in the strength, and perhaps the timing, of when and how they affect perinatal mental health symptoms in men versus women. For women, because the pregnancy period is filled with change and reorganization at several levels—physical, hormonal, and psychological—this may also be a time that cues increased reflection on how to leverage love and support from childhood to care for the new baby, particularly for those with childhood adversity. Accordingly, BCEs may be more salient for women’s mental health than men’s mental health during the pregnancy period. For men, however, the greatest reorganization—and the time of strongest reflection on how to provide loving care—may come after birth, when they meet their new baby. Therefore, it is possible that BCEs will have a stronger effect on fathers’ mental health in the postnatal period, an important question for future study.
Participant Reflections
At the end of the study, participants are encouraged to reflect on how they feel after completing the study and what the experience was like for them. Participants’ reflections thus far illustrate four primary themes, including the experience of participating as therapeutic, the value of contributing to science and generating knowledge, gaining insight about one’s current romantic relationship, and learning from past experiences (see Table 3, p. 50, for examples). Fathers’ reflections in many ways mirrored mothers’ reflections, however some important differences enhance our understanding of family well-being during pregnancy.
Table 3. Example Reflections on Four Primary Themes
| Theme | Pregnant Women | Fathers-to-Be |
|---|---|---|
| Participation as Therapeutic | “I personally liked that I could share some of my life with someone because I have bottled it up for so long. For you all to take interest…made me feel more secure about my life and changes. Thank you. Made me really think.” | “My experience with this study was great. I felt like I let a lot out that had to come out, and I learned something new about myself.” |
| Contributing to Science/Helping Others | “The facilitators were patient and explanatory and made it a comfortable experience. It was good to know my answers and experiences may help the area of psychology.” | “I feel super great about this study. The experience was amazing because I got to voice my opinions and also because I know my study is going to help others in a positive way!” |
| Insights About Current Relationship | “[This study] gave my partner and I the chance to have a moment where we talk to each other about something we don’t always talk about in depth, which makes us a little closer.” | “I enjoyed the study. It allowed me to address factors in my relationship with my child’s mother that have created a lot of drama and stress in our family’s household. My experience went very well and I can definitely see the need for the information that was gathered.” |
| Learning From Past Experiences | “I enjoyed the study as it made me reflect on my own childhood and how it relates to my current pregnancy and motherhood. It also made me visualize the baby more and reflect on my relationship with my partner/father of the baby.” | “I felt great to actually spend time thinking of my past because I don’t do that often, and I’m happy we talked about it as it helped me understand a few things more.” |
Participating as Therapeutic
Pregnant women and fathers-to-be alike described the research experience as therapeutic. Many described that they were able to talk about things that had been “bottled up” and were not previously disclosed to anyone else. One pregnant woman said, “I got some things out that I have put away inside,” and a father-to-be reflected, “It made me think on certain issues I tried to bury and forget, but after talking about them I was able to cope.” One of the therapeutic benefits of these interviews—and a primary goal of the studies in both cities—is to destigmatize mental health problems or treatment of them, and plant a seed for participants to consider therapy or counseling if desired.
Sharing experiences and emotions in a safe space also resulted in feelings of relief, new insights about oneself, and increased hope for the future. A father-to-be stated, “This was a good way to talk and not feel guilty [about] my emotions. Thank you for being open to listen.” Another woman said, “…To be able to talk about a lot of feelings surrounding this pregnancy and my marriage that I hadn’t necessarily taken the time to ponder on…made me feel more confident about things moving forward.” These reflections call for increased opportunities for pregnant women and fathers-to-be to participate in supportive, validating assessments of well-being, both in research and primary-care contexts. These opportunities may be particularly important for fathers-to-be, for whom evidence-based interventions are lacking (Lee et al., 2018).
Contributing to Science/Helping Others
Participants also appreciated the opportunity to benefit other families by generating knowledge and contributing to science. They expressed hope that the information shared was helpful, and appreciation for advancing the field of psychology. A father-to-be noted, “This study will improve understanding of pregnancy and how we change to be better for ourselves and for our children. I think a lot of benefit can come from this.” One pregnant woman also remarked that she was “leaving with a full heart knowing this will help others.” These reflections underscore the strength of the researcher–participant partnership and the extent to which women and men felt their disclosures were valued.
Gaining Insight About Current Romantic Relationships
Participants often reflected on how they gained a deeper understanding of their partners’ perspectives, thereby opening channels of communication and identifying areas for improvement in the relationship. Of note, more men’s than women’s reflections contained content about the romantic relationship, and about half of men’s relationship-related reflections focused on the benefit derived from talking to their partner during the study. One father-to-be said, “I feel like I was helped to see things better from my wife’s point of view.” This finding suggests that a structured, facilitated conversation between partners, even if brief, may lead to noted improvements in communication that are particularly valuable for men. Two other fathers-to-be remarked, “This study may have opened up a lost channel of communication between [my partner] and me” and “It started a dialogue that really needed to begin between us.” Opportunities for both sexes to reflect on their relationship individually and as a couple are beneficial during the pregnancy period.
Learning From Past Experiences
A final theme was that participation facilitated learning from past experiences. One pregnant woman said, “Had a personal breakthrough about my mom. Helped me look at things differently.” Pregnancy is a period when memories of past experiences, especially those of childhood care, become particularly salient for pregnant women (Slade & Cohen, 1996), but less is known about how fathers-to-be consider their past experiences when preparing for fatherhood. One father-to-be said, “Wonderful experience. Brought back some memories I wouldn’t want to remember, but it shows how much one can grow from his past…Thank you. Many can grow from this.” This reflection illustrates that insight from allowing oneself to recollect past experiences can be helpful even if this process is also painful. It also suggests that many individuals may not realize the value of this exercise unless given the opportunity.
In sum, participants’ reflections support in-depth, therapeutic research interviews as a meaningful way to learn about women’s and men’s adjustment during the pregnancy period. These reflections also elucidate the importance of encouraging understanding of how past relationships and experiences are carried forward to affect well-being. One woman said, “I liked this study because I understand more about my unhealthy relationship from the past and the healthier relationship that I now have with my fiancé. I will recommend this study to new mothers-to-be!” Services that facilitate reflection on past experiences and discussion between partners in a safe and validating setting will support families to cultivate existing relationships and provide their new babies with a safe and nurturing environment.
Conclusions
Including fathers-to-be in therapeutic perinatal research has far-reaching benefits. Men provide a much-needed, but rarely investigated, complimentary perspective on how they begin to develop a paternal identity before their baby is born. One father-to-be remarked, “It’s nice to be able to tell my side of what fatherhood is like for me.” Equally important as the therapeutic benefits for participants and invaluable knowledge to the scientific community is the observation that participating women and men actually enjoy this research experience. One man enthusiastically reflected, “I feel great about the study. I enjoyed every bit of it. I would say it was very interesting and fun.” A pregnant woman shared, “I loved opening up more about my feelings, pregnancy, and my love for my husband and children.”

Sharing experiences and emotions in a safe space also resulted in feelings of relief, new insights about oneself, and increased hope for the future. Photo: Halfpoint/shutterstock
As a shadow to these positive reflections, this study also reveals that pregnant women and fathers-to-be continue to be burdened by mental health problems and various layers of stress and trauma despite feelings of hope and optimism. Furthermore, even though this study prioritizes uncovering BCEs as resources for individuals to leverage against ongoing hardship, we must also consider participants who never had certain BCEs. For instance, although 89% of fathers-to-be reported they had at least one caregiver with whom they felt safe during childhood, and 93% had opportunities to have fun at some point while growing up, 11% and 7% of fathers-to-be, respectively, did not have a safe caregiver or any time when they recalled having fun from birth to 18 years old. Although in the minority, these individuals are likely among those in greatest need of resources and support.
Future perinatal research should continue to be supportive and inclusive of diverse families and use therapeutic assessment of positive life experiences to outweigh the burden of working through painful experiences and symptoms during pregnancy. Insight is also continually needed on how to best support families in which both parents may be carrying legacies of unresolved childhood trauma, cumulative stress, and ongoing mental health problems. This study illustrates that pregnant women and fathers-to-be acknowledge that confronting stress and hardship is challenging, but also rewarding and worthwhile if paired with reflection on positive experiences and relationships. Lessons learned from this study will continue to inform how the benefits of BCEs may extend to the postnatal period and how to optimize opportunities for pregnant women and fathers-to-be to reflect upon and recover from adversity to give their babies the healthiest possible beginnings.
Learn More
Safer Beginnings: Perinatal Child–Parent Psychotherapy for Newborns and Mothers Exposed to Domestic Violence
A. F. Lieberman, M. A. Díaz, & P. Van Horn. (2009)
ZERO TO THREE Journal, 29(3), 17–22
Benevolent Childhood Experiences (BCEs) in Homeless Parents: A Validation and Replication Study
J. S. Merrick, A. J. Narayan, C. E. DePasquale, & A. S. Masten (2019)
Journal of Family Psychology. doi: 10.1037/fam0000521
Making Sense of the Past Creates Space for the Baby: Perinatal Child–Parent Psychotherapy for Pregnant Women With Childhood Trauma
A. J. Narayan, G. Oliver Bucio, L. M. Rivera, & A. F. Lieberman (2016)
ZERO TO THREE Journal, 36(5), 22–28
Adverse Childhood Experiences and Risk of Paternity in Teen Pregnancy
R. F. Anda, D. P. Chapman, V. J. Felitti, V. Edwards, D. F. Williamson, J. B. Croft, J. B., & W. H. Giles (2002)
Obstetrics & Gynecology, 100, 37–45. doi: 10.1016/S0029-7844(02)02063-X
Acknowledgment
Funding to support this study comes from the Society for Research in Child Development Grant for Early Career Scholars and the Public Impact Fellowship from the University of Denver. The authors wish to thank all participating families who shared their time and their stories with us. Correspondence concerning this article should be addressed to Angela J. Narayan, Department of Psychology, University of Denver, 347 Frontier Hall, 2155 S. Race St., Denver, CO 80208. Email: Angela.Narayan@du.edu
Authors
Angela J. Narayan, PhD, is an assistant professor in the clinical child psychology doctoral program at the University of Denver and an assistant adjunct professor in the Department of Psychiatry at the University of California, San Francisco (UCSF). She completed her doctoral training in clinical child psychology at the Institute of Child Development, University of Minnesota, and her postdoctoral training at the Child Trauma Research Program within the Department of Psychiatry at UCSF. Her research focuses on developmental psychopathology, childhood trauma, perinatal and infant mental health, and resilience. One of her current research directions focuses on understanding how the prenatal period is a key turning point to buffer the intergenerational transmission of risk in pregnant women and fathers-to-be with histories of childhood trauma and promote resilience in parents and infants.
Victoria M. Atzl., MA, is in her third year at the University of Denver’s clinical child psychology doctoral program. She obtained her bachelor’s degree in human development from Cornell University and her master’s degree in clinical child psychology from the University of Denver. She is primarily interested in the long-term and intergenerational consequences of traumatic experiences, particularly childhood maltreatment, and how the perinatal period can act as an opportune window to disrupt the transmission of adversity.
Jillian S. Merrick is a second-year clinical child psychology doctoral student at the University of Denver. She received her bachelor’s degree in psychology from Macalester College. Her research focuses on the role of protective factors, such as positive childhood experiences and parenting, in promoting resilient outcomes for families experiencing adversity. She is also interested in how parents can capitalize on these protective influences to promote the intergenerational transmission of resilience for their children.
Laura M. River, MA, is a second-year doctoral student in clinical child psychology at the University of Denver. She completed her bachelor’s degree in psychology at Pomona College and her master’s degree in clinical child psychology at the University of Denver. Her research focuses on factors that promote sensitive parenting and child well-being, with particular interest in how interventions targeting prenatal mental health and romantic relationship quality might strengthen the emerging parent–child relationship.
Rachel Peña, MS, is the research project manager for obstetrics and gynecology at Denver Health & Hospital Authority in Denver, CO. She completed her bachelor’s degree in biology at The Ohio State University and her master’s degree in clinical research administration at Central Michigan University. Her research interests include promoting healthy relationships among pregnant women and families, perinatal maternal mental health, and interventions in prenatal and postnatal care to increase the health of the maternal–fetal and maternal–infant bond.
Suggested Citation
Narayan, A. J., Atzl, V. A., Merrick, J. S., River, L. M., & Peña, R. (2019). Therapeutic perinatal research with low-income families: Leveraging benevolent childhood experiences (BCEs) and fathers' perspectives to promote resilience. ZERO TO THREE Journal, 39(5), 43–53.
References
Astone, N. M., & Peters, E. H. (2014). Longitudinal influences on men’s lives: Research from the Transition to Fatherhood Project and beyond. Fathering, 12, 161–173. doi : 10.3149/fth.1202.161
Atzl, V. M., Grande, L. A., Davis, E. P., & Narayan, A. J. (2019). Perinatal promotive and protective factors for women with histories of childhood abuse and neglect. Child Abuse & Neglect, 91, 63–77. doi: 10.1016/j.chiabu.2019.02.008
Atzl, V. M., Narayan, A. J., Rivera, L. M., & Lieberman, A. F. (2019). Adverse childhood experiences and prenatal mental health: ACEs type and age of maltreatment onset. Journal of Family Psychology. doi: 10.1037/fam0000510
Bunting, L., & McAuley, C. (2004). Research review: Teenage pregnancy and parenthood: The role of fathers. Child & Family Social Work, 9, 295–303. doi: 10.1111/j.1365-2206.2004.00335.x
Cabrera, N. J., Karberg, E., & Kuhns, C. (2017). Minority fathers and children’s positive development in the United States. In N. J. Cabrera & B. Leyendecker (Eds.), Handbook on positive development of minority children and youth (pp. 197–216). New York, NY: Springer.
Centers for Disease Control and Prevention. (2016). Adverse childhood experiences (ACEs). Source link
Clinton, J. F., & Kelber, S. T. (1993). Stress and coping in fathers of newborns: Comparisons of planned versus unplanned pregnancy. International Journal of Nursing Studies, 30, 437–443.
Cox, J. L., Holden, J. M., & Sagovsky, R. (1987). Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. The British Journal of Psychiatry, 150, 782–786.
Earls, M. F. (2010). Incorporating recognition and management of perinatal and postpartum depression into pediatric practice. Pediatrics, 126, 1032–1039.doi: 10.1542/peds.2010-2348
Ellis, B. J., Bates, J. E., Dodge, K. A., Fergusson, D. M., John Horwood, L., Pettit, G. S., & Woodward, L. (2003). Does father absence place daughters at special risk for early sexual activity and teenage pregnancy? Child Development, 74, 801–821. doi: 10.1111/1467-8624.00569
Fagan, K. (2016, June 26). SF homeless problem looks the same as it did 20 years ago. San Francisco Chronicle. Source link
Finer, L. B., & Zolna, M. R. (2011). Unintended pregnancy in the United States: Incidence and disparities, 2006. Contraception, 84, 478–485. doi: 10.1016/j.contraception.2011.07.013
Garfield, C. F., Duncan, G., Rutsohn, J., McDade, T. W., Adam, E. K., Coley, R. L., & Chase-Lansdale, P. L. (2014). A longitudinal study of paternal mental health during transition to fatherhood as young adults. Pediatrics, 133, 836–843. doi: 10.1542/peds.2013-3262
Lee, J. Y., Knauer, H. A., Lee, S. J., MacEachern, M. P., & Garfield, C. F. (2018 online). Father-inclusive perinatal parent education programs: A systematicreview. Pediatrics, 142. doi: 10.1542/peds.2018-0437
Narayan, A. J., Rivera, L. M., Bernstein, R. E., Castro, G., Gantt, T., Thomas, M.,Nau, M., Harris, W. W., & Lieberman, A. F. (2017). Between pregnancy and motherhood: Identifying unmet mental health needs in pregnant women with lifetime adversity. ZERO TO THREE Journal, 37(4), 14–23.
Narayan, A. J., Rivera, L. M., Bernstein, R. E., Harris, W. W., & Lieberman, A. F.(2018). Positive childhood experiences predict less psychopathology and stress in pregnant women with childhood adversity: A pilot study of the benevolent childhood experiences (BCEs) scale. Child Abuse and Neglect, 78, 19–30. doi: 10.1016/j.chiabu.2017.09.022
National Center for PTSD (2017). PTSD checklist for DSM-5 (PCL-5). Source link
Ramchandani, P., Stein, A., Evans, J., O’Connor, T. G., & ALSPAC Study Team. (2005). Paternal depression in the postnatal period and child development: A prospective population study. The Lancet, 365, 2201–2205. doi: 10.1016/S0140-6736(05)66778-5
River, L. M., Narayan, A. J., Atzl, V., Rivera, L. M., & Lieberman, A. F. (2019). Romantic partner support during pregnancy: The discrepancy between self-reported and coder-rated support as a risk factor for prenatal psychopathology and stress. Manuscript in preparation.
Salvatore, J. E., Kuo, S. I. C., Steele, R. D., Simpson, J. A., & Collins, W. A. (2011). Recovering from conflict in romantic relationships: A developmental perspective. Psychological Science, 22, 376–383. doi: 10.1177/0956797610397055
Seng, J. S., Rauch, S. A., Resnick, H., Reed, C. D., King, A., Low, L. K., … & Liberzon, I. (2010). Exploring posttraumatic stress disorder symptom profile among pregnant women. Journal of Psychosomatic Obstetrics & Gynecology, 31, 176–187. doi: 10.3109/0167482X.2010.486453
Settersten, R. A., Jr., & Cancel-Tirado, D. (2010). Fatherhood as a hidden variable in men’s development and life courses. Research in Human Development, 7, 83–102. doi: 10.1080/15427609.2010.481520
Slade, A., & Cohen, L. J. (1996). The process of parenting and the remembrance of things past. Infant Mental Health Journal, 17, 217–238. doi: 10.1002/(SICI)1097-0355(199623)17:3<217::AID-IMHJ3>3.0.CO;2-L
Sperlich, M., & Seng, J. S. (2008). Survivor moms: Women’s stories of birthing, mothering and healing after sexual abuse. Eugene, OR: Motherbaby Press.
Weathers, F. W., Litz, B. T., Keane, T. M., Palmieri, P. A., Marx, B. P., & Schnurr, P. P. (2013). The PTSD checklist for DSM-5 (PCL-5). Source link